170 Commonwealth Avenue, Suite 101 Boston, MA 02116
Phone: (617) 726-5280
Making Concave Faces Convex
Concave faces are often considered less attractive than convex ones. The lesser midface skeletal projection intrinsic to concave faces poorly supports the soft tissues resulting in premature lower lid and cheek descent, as well as visible bags.  These faces are “morphologically prone†to further lower lid descent after blepharoplasty.  The concave midface also makes the eyes and nose appear prominen
Severe midface concavity is often seen with the craniofacial dysostoses of Apert and Crouzon. It may not only result in occlusal disharmony, but also compromises globe protection and airway adequacy. Patients with this morphology require skeletal osteotomies usually at the LeFort III and sometimes, at the LeFort I level to remedy ocular, respiratory, and occlusal dysfunction as well as to improve facial aesthetics.
Less severe midface hypoplasia is a common facial skeletal variant. In patients with this morphology; occlusion is normal or has been compensated by orthodontics. They have neither respiratory nor ocular compromise. It is in this population that midface skeletal augmentation with multiple implants can simulate the visual effects of skeletal osteotomy and advancement.
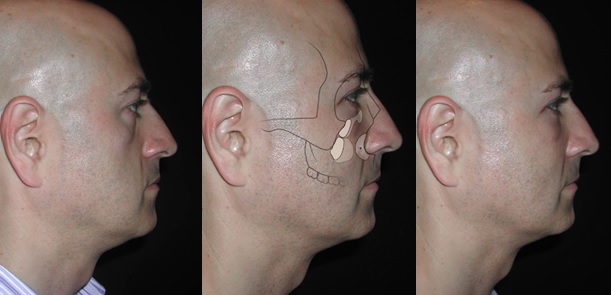
As shown above, the implants used to effect these changes include ones that augment the infraorbital rim,  the piriform appeture,  and the malar area. These implants are all modified so as to meet the specific needs of the patient. Multiple implants are used so that the infraorbital nerve is not compromised and so that the complex curvature of the skeleton can be mimicked.
The surgery is performed by first gaining access to the midface skeleton through lower lid and intraoral incisions. The entire midface is freed in the subperiosteal plane. The midface skeleton is augmented with a combination of porous polyethylene implants immobilized with screws. The midface soft tissue envelope is elevated and fixed with sutures tied to the infraorbital rim, implant and/or the lateral orbital rim.
Patients with midface concavity have an underlying deficiency in maxillary and zygomatic skeletal projection. Ptosis of the cheek and lower lid is accelerated by the lack of skeletal support in this patient population. Facial skeletal augmentation with multiple screw fixed alloplastic implants, together with subperiosteal midface soft tissue elevation, can normalize and enhance the appearance of these patients.  The technique described here is effective and avoids problems inherent in other methods used to produce midface convexity.
If skeletal midface deficiency is accompanied by Class III malocclusion,  LeFort osteotomy, (sometimes at two levels) is required to normalize occlusion and to improve globe- rim relations. In skeletally deficient patients whose occlusion is normal or has been previously normalized by orthodontics, skeletal repositioning would necessitate additional orthodontic tooth movement. Such a treatment plan is time consuming, costly, and potentially morbid. It is, therefore, appealing to few patients.
The projection of the midface skeleton can be increased by augmenting it with autogenous bone or alloplastic materials. Aesthetic skeletal augmentation is rarely done with autogenous bone because of the unpredictability of the result. Once the graft is revascularized by the host, it becomes subject to osteoclastic activity as determined by mechanical load and soft tissue deforming forces (Wolff’s law). In addition, graft harvest is painful and time consuming. It increases both operating time and recovery time and therefore increases cost. Alloplastic augmentation of the facial skeleton avoids the unpredictability and morbidity inherent in the use of autogenous materials.
This author prefers to augment the concave midface skeleton with multiple implants of porous polyethylene that are fixed with screws. In certain situations, implants that are computer designed specifically for the patient are used. The implants are fixed with screws for the following reasons. Screw fixation immobilizes the implants. This eliminates any intra or postoperative implant movement and subsequent undesirable contour. Their rigid immobilization allows the implants to be contoured “in place†so that there is in imperceptible transition between the implant and the skeleton. Finally, screw fixation allows the posterior surface of the implant to be applied to the anterior surface of the facial skeleton thereby obliterating any gaps between these two surfaces. Gaps result in an unanticipated increase in projection equivalent to the gap space.
Free fat grafting can be an effective means of augmenting facial contour. This technique is intuitive for the restoration of soft tissue volume loss due to senile atrophy. In my experience, fat injection has a limited role in simulating the effect of an increase in skeletal projection. Whereas augmenting the facial skeleton results in an increase in the projection of the soft tissue envelope, augmenting the soft tissue volume results in an inflation of the soft tissue envelope. Over augmentation of either component brings home the point. If overly large implants were placed on the skeleton, the appearance would be too defined and ultimately, skeletal. If too much fat were placed in the soft tissue envelope, an increasingly spherical and otherwise undefined shape would result.
Repositioning midface soft tissues has several benefits. It restores cheek fullness, recreates a cheek-lid interface with a relatively shortened lower lid while narrowing the palpebral fissure shape by raising the lower lid margin.
Leave Comments
You must be logged in to post a comment.