170 Commonwealth Avenue, Suite 101 Boston, MA 02116
Phone: (617) 726-5280
Subperiosteal and Full-Thickness Skin Rhytidectomy
Face lift surgery is rejuvenative cosmetic surgery and, therefore, by definition [L. juvenis, young person)],1 its goal is to restore a youthful appearance. Successful face lift surgery re- quires that the plastic surgeon recognize the attributes of the youthful face and that he develop effective techniques to restore them. Iatrogenic sequelae should not detract from this goal. This study presents an approach for simultaneous rejuvenation of all three of the horizontal zones of the face—the upper, middle, and lower face. This requires four basic maneuvers, including a subperiosteal brow and midface lift using coronal and intraoral approaches; upper lid blepharoplasty; trans- conjunctival retroseptal lower lid fat excision and skin-only blepharoplasty; and a lower face lift whereby full-thickness skin and subcutaneous flaps are elevated, tailored, and re positioned. The aesthetic goals, the operative techniques, and their rationale are   presented.
AESTHETICÂ GOALS
The goal of face lift surgery is to restore youthful contours to the face. Certain anthropometric studies2 and recent computerized tomography-based studies3 have quantified the characteristics and relations of many facial features in young adults. This objective data, together with longstanding subjective tenets of the cosmetic industry,4 can help guide the surgeon in rejuvenating the face. Ideally, this surgery should be free of any face lift sequelae.5 Iatrogenic stigmata associated with rejuvenative cosmetic surgery include: the lateral sweep,5 the elevated and widened medial brow,6,7 the distorted palpebral fissure,8,9 and the over-operated neck.10 The major aesthetic goals for each horizontal third of the face are described.
Upper Third
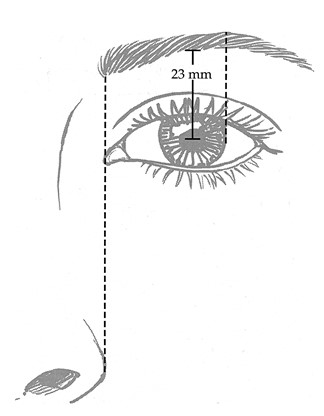
Restoring the position and shape of the brow (Fig. 1) is the major goal in the rejuvenation of the upper third of the face. In the young, attractive woman, the brow should rest just at the supraorbital rim. The highest point of the brow should lie at the junction of the middle and lateral third of the brow or at approximately the lateral border of the iris. The medial extent ends on a vertical line drawn through the medial canthus and the lateral aspect of the alar base. The arch of the brow should flow into the curve of the nasal side wall.4,6,11 This shape has been described as an apex lateral slant.6 When measured from mid- pupil to lower edge of the brow, the average height of the brow in young female adult is 23 ± 3 mm.2 Ideal brow height determined by the subjective analyses of other workers12–14 is similar to the anthropometric measurement.2
In addition to restoring the shape and position of the brow, its elevation improves upper lid contour by removing some upper lid skin redundancy. Brow elevation also lessens the severity of transverse forehead wrinkles.15
Middle Third
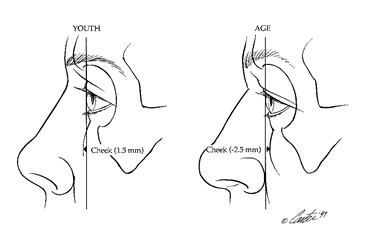
Repositioning the cheek is the major goal of middle-third rejuvenation. The loss of cheek prominence that occurs with aging has been documented. Using three-dimensional, reformatted, computerized tomographic scans, Pessa et al.3 compared the projection of the cheek prominence relative to the anterior surface of the cornea in young and old patients (Fig. 2). In the youthful face, the cheek mass was positioned an average of 1.5 mm anterior to the cornea. This relationship was termed a positive vector. In older individuals, the cheek mass was positioned an average of 2.5 mm posterior to the cornea. This relationship was termed a negative vector. The change in anterior cheek mass relative to the corneal surface with aging was statistically significant (p = 0.0038). This vector change resulted not only from soft-tissue descent but also from a retrusion of the infraorbital rim due to the remodeling of the craniofacial skeleton that occurs with age.
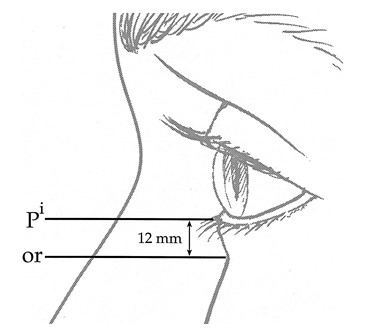
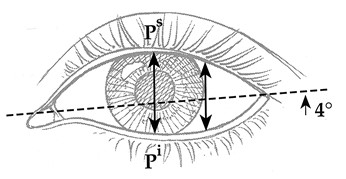
In addition to restoring the cheek prominence, cheek elevation softens the nasolabial fold and repositions the cheek-lid interface, effectively shortening the height of the lower lid.16 Elevation of the cheek-lid interface not only improves the contour of the lower lid but also maintains or, in some patients, improves the shape of the palpebral fissure. In the young female adult, the lower lid is closely applied to the convexity of the globe to create a concavity before it merges with the convexity of the cheek. This area of merging, or the cheek-lid interface corresponds to the level of the infraorbital rim. The average height of the lower lid in the young female adult is 12 ± 1.3 mm (Fig. 3).2 Descent of the cheek with aging not only lengthens the appearance of the lower lid, but also may also alter the shape of the palpebral fissure by lowering the position of the lower lid margin. In young women, the vertical height of the palpebral fissure at the level of the pupil was measured to be 10.8 ± 1.2 mm. The length of the fissure, measured from me- dial to lateral canthus, is approximately 31 mm. The lateral canthus is located an average of 4 degrees ± 2 degrees higher than the  plane created by the medial canthi (Fig. 4).2 This results in an upward tilt of the fissure and its rapid tapering from midpupil laterally. Lower lid and midface surgery should maintain or improve, that is, narrow the shape of the palpebral fissure.
Lower Third
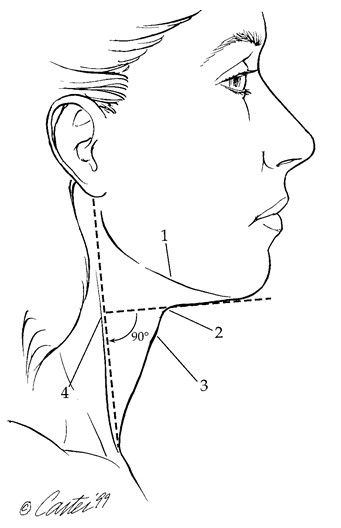
The goal of rejuvenation of the lower one- third of the face is to restore mandibular and cervical-mental contour. Ellenbogen and Karlin17 have proposed visual criteria for restoring a youthful neck. These include a distinct inferior mandibular border, subhyoid depression,  a visible thyroid cartilage bulge, a visible anterior border of the sternocleidomastoid muscle, and a cervicomental angle between 105 degrees and 120 degrees.
These authors pointed out that, because the sternocleidomastoid muscle is always almost vertical, a sternocleidomastoid submental line would be 90 degrees and easy to assess. An adaptation of these criteria is presented in Figure 5. Restoration of these contours requires correction of the jowls, removal of excess submental fat, and correction of platysmal bands. Skeletal anatomy, including the shape and position of the mandible and hyoid may limit the surgeon’s ability to reach these aesthetic goals with face lift surgery alone.
Summary
The wide range of facial morphology, the degenerative changes that occur with time to connective tissues, and the limitations of  surgery have made transformation of the anthropometric relationship of an aged face to the ideal or average measurements of youth unrealistic.
However, using these anthropometric “ideals†allows a more objective, goal-oriented, preoperative, and postoperative assessment of rejuvenative surgery. The scientific definition of a youthful face can be summarized as one having brows with an apex, lateral slant; short lower lids; narrow eyes; full cheeks; and a well- defined neck and mandibular border. The cover of virtually every fashion magazine shows young models whose faces have these attributes. A face with these attributes should, therefore, be the goal of face lift surgery.