170 Commonwealth Avenue, Suite 101 Boston, MA 02116
Phone: (617) 726-5280
The Safe Zone for Placement of Chin Implants
Alloplastic chin augmentation is the most commonly performed facial skeletal augmentation procedure in the United States.1 Despite its acceptance and popularity, chin augmentation carries a significant number of complications,
including underaugmentation or overaugmentation, malpositioning, infection, extrusion, bone resorption, nerve injury, and chin ptosis.2,3 Certain complications are simply unavoidable, while others can be attributed to poor patient selection or a technical error.
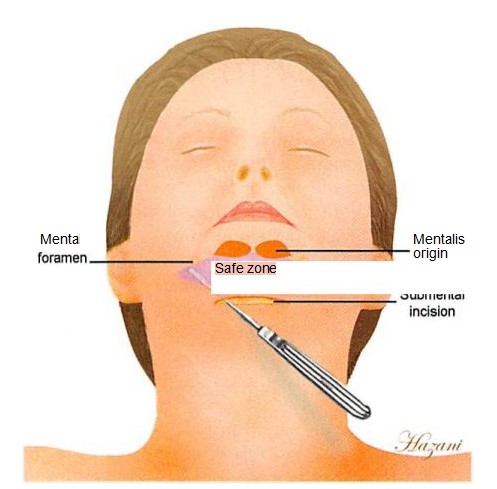
The risk for technical errors increases when the limits of the dissection are unclear or when the surgeon is unfamiliar with the topography and surface anatomy of the mandible. In a standard submental approach, dissection proceeds in the subperiosteal plane along the anterior mandible. Above the mental protuberance, the upper limit of the dissection is the origin of the mentalis muscle. Laterally, the mental foramen is identified below the root of the second premolar and the exiting nerve is preserved.4
The purpose of this anatomic study was to define a safe zone of dissection along the anterior surface of the mandible by predicting the location of the mentalis origin and the mental foramen (Fig. 1). A zone of safety can facilitate a more reliable approach for the placement of chin implants and avoid the complications of lower lip incompetence or lower lip paresthesia.
METHODS
Fourteen fresh cadaveric hemifaces were dissected with the aid of loupe magnification. Dental anatomic landmarks were used to identify the mentalis muscle origin and the mental foramen on a horizontal axis below the alveolar ridge. Distances were then measured from the inferior border of the mandible to the mentalis muscle and the mental foramen to construct the zone of safety. The origin, insertion, and shape of the mentalis muscle were then inspected, as various cadaveric studies have indicated conflicting findings regarding its anatomic description.
RESULTS
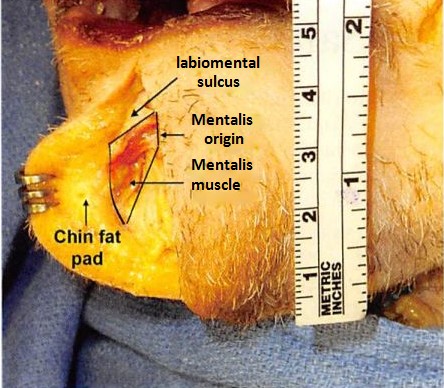
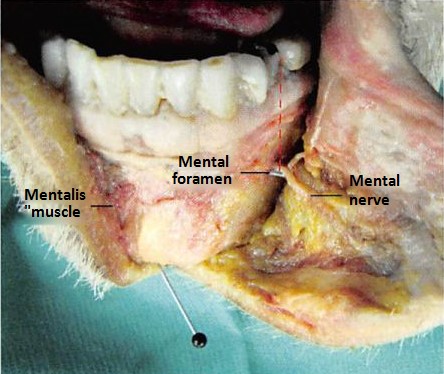
The mentalis was identified as a fan-shaped muscle originating from the alveolar process below the incisors roots and inserting into the chin just below the labiomental sulcus (Fig. 2). The mental foramen was found most commonly at the level of and below the roots of the first and second premolars (Fig. 3). The mentalis muscle and the mental foramen were 1.8 ± 0.3 cm and 1.5 ± 0.2 cm cephalad to the inferior border of the mandible, respectively. These distances defined the borders of the safe zone above the mandibular border (Fig. 4).
DISCUSSION
Mental Nerve Morbidity
It is difficult to estimate the exact incidence of mental nerve paresthesia in aesthetic surgery of the chin, but in the orthognathic literature, paresthesia following osseous genioplasty ranges from 3.4 percent to 12 percent.3,5-7 Chin hypesthesia, dysesthesia, or paresthesia following alloplastic chin augmentation can be caused by direct damage to the nerve from a scalpel,2 by compression of the nerve against a malpositioned implant,2,3 or potentially by damage to the inferior alveolar nerve from stabilizing screws that are placed too cephalad along the mandibular border.
Mental Nerve Anatomy
Historically, it was believed that the course of the inferior alveolar nerve comes directly out of the mental foramen in a straight horizontal projection from its posterior course. Hwang et al.8 have recently reevaluated the anatomy of the inferior alveolar nerve, the mental nerve, and the mental foramen. The terminal mandibular canal is located at an average of 4.5 mm under the mental foramen, advances 5 mm anteriorly, loops, and ends at the foramen. The horizontal position of the mental foramen is below the second mandibular premolar or in the interdental space between the first and second premolar teeth in the overwhelming number of subjects.9-12
On the vertical axis, the mental foramen is located approximately 1.5 cm above the mandibular border. This is consistent with measurements reported by Smajilagic and Dilberovic9 in which vertical distances were taken from 150 Bosnian mandibles and were estimated to be 1.4 cm. We preferred the use of distance measurements to the use of distance ratios, as reported in other anatomic studies 9,11 In addition, measured distances from the mental foramen to the alveolar ridge were not a clinically useful tool in this study. Since the alveolar ridge is not visualized in a routine submental approach, it cannot be used as a landmark.
Mentalis Muscle Morbidity
The cause for mentalis muscle dysfunction after chin surgery depends on the surgical approach. If an intraoral access is used, damage is likely to occur when the muscle is divided or stripped from the mandible to facilitate exposure for placement of an extended implant.1:5 Zide14 maintains that in the routine intraoral procedure for chin implantation, the mentalis muscle’s origins are always traversed. When a submental access is used for chin augmentation, overaggressive soft-tissue dissection can result in mentalis origin displacement.15
We occasionally see mentalis dysfunction after orthognathic surgery and rarely after alloplastic chins augmentation. It is very possible that some, if not most, of the complications are related to dissection in the wrong plane. The safe zone defines the anatomic landmarks for such dissection in the subperiosteal plane and the upper limits of the dissection in the central portion of the anterior mandible. The zone of safety is meant to serve as a guide for the novice surgeon, since the incidence of chin augmentation is on the rise (71 percent in 2011),1 and we are likely to see more complications if attention is not given to these structures.
Mentalis Muscle Anatomy
The mentalis muscles are a pair of fan-shaped structures joined in the midline. They are separated from each other by a firm septum, and occasionally they have some fat overlying them at the sulcal origin.15 The mentalis muscle originates from the alveolar process of the mandible below the incisors roots. This compact, circular origin fans out to a more dispersed insertion in the chin. Since the lower muscle fibers pass obliquely down-ward, an attempt to contract the mentalis muscles will result in elevation of the lower lip.15 When an intraoral approach is used, in aesthetic or reconstructive cases, and the mentalis is divided, it should be reapproximated. Failure to re-approximate the mentalis fibers intraoperatively can lead to chin ptosis, lip ptosis, drooling, and an increase in lower teeth show.3
Correction of iatrogenic chin ptosis and mentalis muscle dysfunction can be difficult and demanding. One technique, which has demonstrated moderate success, is die original mentalis reefing procedure. It has since been modified and improved with supraplacement of anchor sutures at the highest mentalis origin position.15 Cases of mild ptosis can be corrected by excising submental soft tissue through an elliptical submental incision,3 but these excisions proride no solution to the problem of mentalis strain and lower teeth show.
CONCLUSIONS
A safe zone of dissection for alloplastic chin augmentation is identified. The strength of this study is in its applicability in reconstructive, aesthetic, and orthognathic surgery of the mandible. Although it is more difficult to discern the limits of the dissection from an intraoral access, we believe that this zone of safety can be used as a guide in both submental and intraoral approaches.