Refining Post-orthognathic Surgery Facial Contour with Computer Assisted Designed/Computer Assisted Manufactured (CAD/CAM) Implants
Orthognathic surgery is routinely performed to correct significant dentofacial deformities. The most frequently performed procedures are Le fort I maxillary osteotomies and sagittal split mandibular osteotomies. With proper surgical and orthodontic planning and execution, dental malocclusion can be corrected and facial disharmonies improved. However, multidimensional repositioning of the maxillofacial skeleton may create new contour irregularities and abnormalities, especially with movements of large magnitude and for correction of pre-existing facial asymmetries. Both the midface and lower face can manifest characteristic post orthognathic contour irregularities. This imbalance is proportionate to the magnitude of sagittal skeletal advancement.
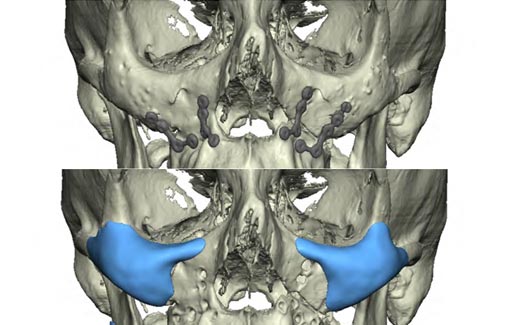
Since the Le Fort I maxillary osteotomy and advancement is performed beneath the infraorbital foramen, the midface skeleton above the foramen maintains its projection while the lower portion moves forward as shown in the illustration. The overlying soft tissues are also advanced with the lower skeleton. As a result, the cheeks now appear low as shown in the patient who had the illustrated LeFort I advancement.



Lower Face Contour
Sagittal split osteotomy of the deficient mandible with advancement in the sagittal plane may result in ramus asymmetry and border irregularities to varying degrees as shown in this model of a patient who had undergone sagittal split osteotomy and sliding genioplasty.
Ramus asymmetry immediately after surgery occurs when the surgeon fails to create similar osteotomies and maintain similar osteotomy gaps (with rigid fixation) on both sides. The surgeon has little or no control over the relationship of the proximal and distal fragments because the condyle must be positioned in its fossa and the body must be positioned to correct the occlusion. The positioning of these two areas dictates ramus and angle position. Rigid fixation has virtually eliminated these problems related to inadequate fixation, but contour abnormalities may still occur due to incorrect positioning with resultant counterclockwise rotation or after very large movements.
Border irregularities result from gaps at the osteotomy sites after sagittal osteotomy of the mandible or horizontal osteotomies of the chin with advancement. The native mandible anatomy and surgical technique influence the presence and severity of these irregularities
The use of alloplastic implants as an adjunct to orthognathic surgery has been previously presented by this author (Yaremchuk MJ, Doumit G, Thomas MA. Alloplastic Augmentation of the Facial Skeleton: An Occasional Adjunct or Alternative to Orthognathic Surgery: Plast Reconstr Surg. 2011;127(5):2012) Readily available (off the shelf) implants were contoured at the time of surgery to correct the post orthognathicdeformities described above. Post-surgical as well as intrinsic facial asymmetries together with the challenge of hand carving three dimensional implant contours limits facial contour improvement.
Computerized Tomographic (CT) scans
Computer assisted designed/computer assisted manufactured (CAD/CAM) implants has vastly improve the ability to refine facial contour and balance after orthognathic surgery. Dr. Yaremchuk recently published his use of this modality in a recent article - Lee, JH, Kaban, LB, Yaremchuk, MJ. Refining Post–Orthognathic Surgery Facial Contour with Computer-Designed/Computer-Manufactured Alloplastic Implants, Plast. Reconstr. Surg. 142: 747, 2018.)
To produce CAD/CAM alloplastic implants, CT scans with high resolution (<2 mm) are acquired using a recommended protocol. High resolution scans allow individual image slices to be stacked to construct three dimensional images of both the skeleton and soft tissue envelope from the top of the skull to the hyoid bone.
Implant Design
Two options are available for the design process. From the CT data a three dimensional model of the patient’s facial skeleton is manufactured. The surgeon augments the deficient areas on the model with clay. The implant company uses the clay prototypes to manufacture implants. The alternative technique, which Dr. Yaremchuk prefers, involves a web based meeting between the surgeon and the manufacturer’s engineer at which time implants are designed virtually. This method allows millimeter precision in design and measurable relations before the upper and lower face.
Correction of Post-surgical Upper Face Disharmony
The midface disharmony after Le Fort I osteotomy and advancement is a deficiency in the maxilla above the level of the osteotomy. Its custom implant correction always includes the infraorbital rim (the area directly beneath the eye) and the medial aspect of the malar prominence. The amount of its sagittal projection is an aesthetic judgment determined by the amount of lower midface advancement and by the amount of globe prominence.
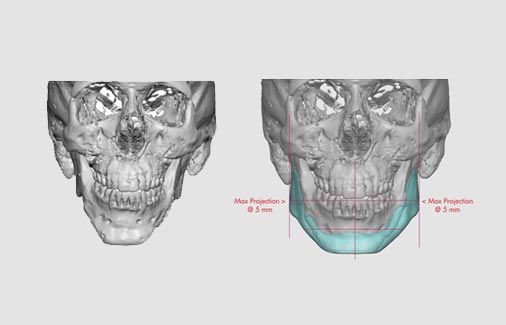
The lower face disharmonies after BSSO include possible asymmetry in lower face height and width as well as border irregularities. If a sliding genioplasty has been performed, border irregularity at the osteotomy sites and chin asymmetry may be present. A grid pattern placed over the image is used to design the implant addressing the central and lateral portions of the mandible separately. Centrally, that is from the midline to the mental foramen, the implant is designed to be symmetric to the midline as determined by the position of the columella and the central incisors. Laterally, gonial angle position is determined by its relation to its respective upper face skeleton rather than the midline. The central and lateral designs are then coordinated to provide a regular inferior mandible border.
Using the biotechnical advances of rigid fixation and bone substitutes to provide reliable expansion of the facial skeleton, Rosen was the first to transition orthognathic surgical goals to become primarily aesthetic. These modalities allowed him to plan his treatment with primarily aesthetic goals of creating convexity, balance and soft tissue support rather than the more typical satisfaction of normative facial relations. The use of CAD/CAM alloplastic implants is another application of biotechnology to add aesthetic refinement to orthognathic surgery.