Blepharoplasty
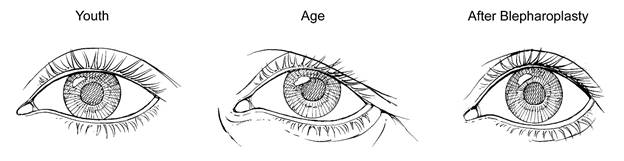
Blepharoplasty, or eyelid surgery, can fix bags, dark circles, droopy eyelids, and tear trough concerns. Dr. Yaremchuk employs several techniques in his eyelid surgeries to restore youthful contour and dimensions to the eyelids. The late medical anthropologist Leslie Farkas documented that the typical youthful eye among a large sample of young North American women had a narrow appearance, upward tilt from the inner to outer aspect, and short lower lid.
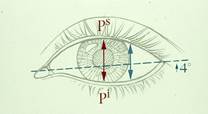
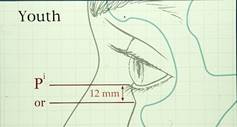
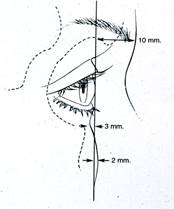
Illustration of Dr. Farkas’ measurements of the youthful eye with narrow fissure, upward tilt and short lower lid.
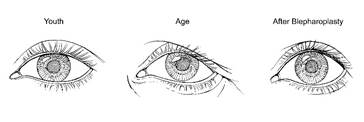
As the eye ages, it takes on a rounder appearance as gravity takes effect and supporting tissues relax over time. Instead of creating the desired youthful effect, too often conventional blepharoplasty techniques exaggerate the aged appearance by resulting in a post-op “round eye” look.
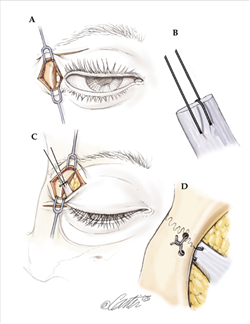
Dr. Yaremchuk employs a variety of innovative techniques depending on the clinical situation. These techniques include the transconjunctival approach with arcus marginalis release and fat redistribution as opposed to excision, selective use of lateral canthopexy, skeletal augmentation and midface elevation. Dr. Yaremchuk has presented and written extensively about these techniques in scholarly articles, book chapters, and lectures.
The tear trough deformity is a challenging problem. It is often associated with "dark circles." Most often, Dr. Yaremchuk corrects the tear trough deformity using the transconjunctival arcus marginalis release with fat transposition. For severe deformities, he employs both the transconjunctival arcus marginalis release with fat transposition and a tear trough implant. The video here shows Dr. Yaremchuk's technique for correcting a severe tear trough deformity.
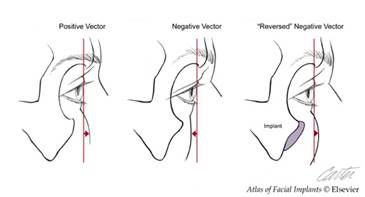
Patients with prominent eyes have long been known to be predisposed to complications after lower lid blepharoplasty. Dr Yaremchuk has developed techniques to improve the appearance of the lower lids in patients with prominent eyes. Eyes appear overly prominent because the upper midface skeleton (the bone directly beneath the eye) lacks projection. Without a projecting skeleton to support it, the lower lid and cheek tissues tend to fall, making the eyes prominent. Dr Yaremchuk treats this problem building up the skeleton with an infraorbital implant and performing a midface lift to elevate the cheek and lower lid tissues on the new, projecting skeletal framework.
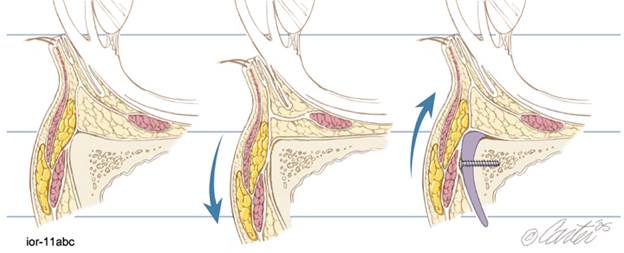
Blepharoplasty for prominent eyes: The illustration shows cross section lateral views of the orbit taken at the level of the pupil. The diagram on the left shows the average relations of the lower lid and globe. The middle illustration depicts a prominent eye due to lack of projection of the skeleton and the subsequent descent of the lower lid and cheek. On the far right, the bone has been augmented with an infraorbital rim implant and the cheek and lid elevated (subperiosteal midface lift). Note how the lid margin rests higher on the globe making the eye appear less prominent.
Dr. Yaremchuk also performs revisional blepharoplasty to correct unfortunate results for patients who underwent prior unsatisfactory blepharoplasty procedures elsewhere.
Dr. Yaremchuk has shared his face and eyelid rejuvenation techniques with plastic surgeons in live surgery demonstrations around the world including Spain, Germany, Russia, Argentina and Taiwan. He has demonstrated his blepharoplasty and skeletal augmentation surgery at the Canadian Society for Aesthetic Plastic Surgery Annual Meeting and at the Annual Atlanta Oculoplastic Symposium.

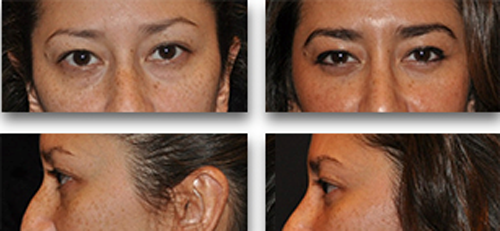
* This Asian patient underwent upper and lower lid blepharoplasty.
* Underwent lower lid blepharoplasty by arcus margnalis release with fat transpositon to correct tear troughs and restore youthful lower lid contour
* Underwent lower lid blepharoplasty by arcus margnalis release with fat transpositon to correct tear troughs and restore youthful lower lid contour
* Underwent lower lid blepharoplasty by arcus margnalis release with fat transpositon to correct tear troughs and restore youthful lower lid contour

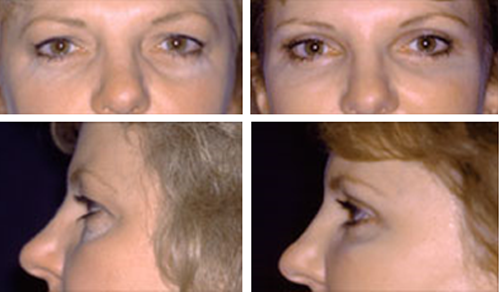
* This patient with prominent eyes underwent orbital decompression, infraorbital rim augmentation, midface lift and medial fat transposition to improve periorbital aesthetics
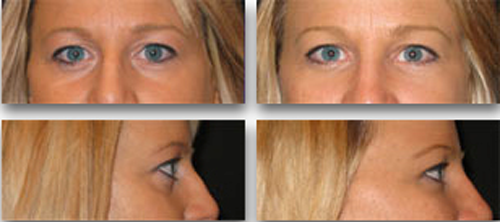
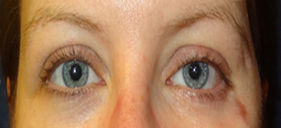
* This patient underwent transconjunctival blepharoplasty with arcus marginalis release and fat transposition.

* This patient with prominent eyes underwent orbital decompression, infraorbital rim augmentation, midface lift and medial fat transposition to improve periorbital aesthetics

* This patient underwent transconjunctival blepharoplasty with arcus marginalis release and fat transposition.

* Underwent upper and lower lid blepharoplasty

* Underwent Asian upper and lower lid bleph

* This Asian patient underwent upper and lower lid blepharoplasty
Surgical Procedures to Reposition the Retracted Lower Eyelid
Background

In addition to the unappealing appearance with increased scleral can include the inability for the eyelids to close (referred to as lagophthalmos), and exposure keratitis. This can lead to dry eye syndrome, ocular discomfort, excessive tearing, photophobia, and blurred vision.
Dr. Yaremchuk utilizes many surgical procedures to correct lower eyelid retraction depending on the periorbital structures involved. Spacer grafts, bridge-of-bone lateral canthopexy, subperiosteal midface lifts and infraorbital rim bone augmentation are all part of his armamentarium. Certain clinical problems require a combination of these procedures to restore lower lid position.
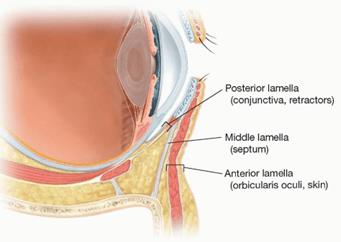
Lower Lid Anatomy
The normal lower eyelid lies at or just above the inferior corneal limbus (the perimeter of the iris).
It is considered a trilamellar structure—the anterior lamella (skin and orbicularis oculi muscle), the middle lamella (orbital septum), and the posterior lamella (lower eyelid retractors and conjunctiva.
The lid is tethered at both ends by its canthal tendons which are attached to the orbit.
The lid is supported by its underlying obital rim.
Deficiency of any layer of this trilamellar structure and its supporting orbital rim can result in lower eyelid retraction.
Spacer Grafts
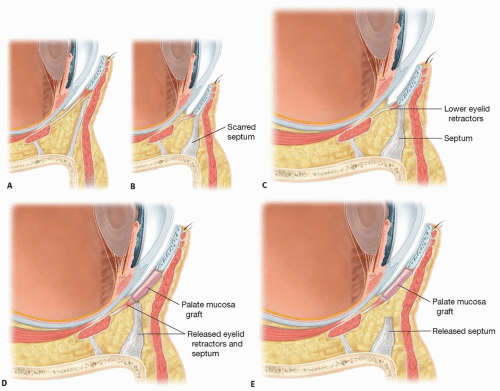
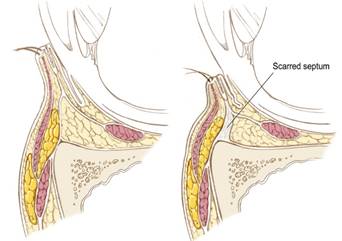
Scarring and subsequent shortening of middle and posterior lamellae most often results after surgical violation to the middle and posterior lamella approaches to expose the orbital anatomy or to correct traumatic orbital injuries or to cosmetically improve intraorbital fat. Traumatic or iatrogenic soft tissue injury or hemorrhage can result in untoward healing with contracture and lamellar shortening.
Correction of posterior and middle lamellar shortening is accomplished by incising the lamellae which results in a space between the edges. The space is then bridged with a graft. The graft effectively lengthens and supports the lamella and hence the lower lid. Palatal mucosa, conchal cartilage and treated alloplastic dermal matrices are all used as spacer grafts.
Subperiosteal Midface Lift
Malposition of the lower lid is a frequent problem after transcutaneous blepharoplasty. Overresection of the lid skin and underlying muscle (outer lamella) with scarring of the orbital septum (middle lamella) causes the lower lid to descend and the lateral canthus to descend medially in a “round eye”. An operation intended to rejuvenate the lower lid unfortunately ages it as shown below.
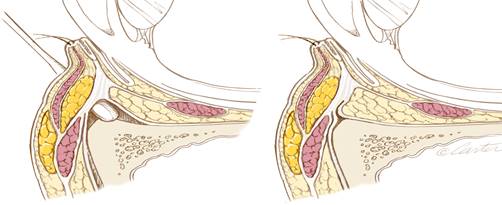
The subperiosteal midface lift is an ideal procedure to correct lower lid malposition due to overresection of the lid skin and underlying muscle. Using intraoral and periorbital incisions, the full thickness of the midface tissues (skin, subcutaneous flat and muscles) are elevated from the underlying skeleton and fixed to the infraorbital rim after scarring in this area is released. The fat from the underlying of the midface tissue supports the lid margin while the elevated midface skin effectively adds skin to the deficient lower lid.
Lateral Canthopexy
The youthful palpebral fissure is long and narrow with a slight lateral upward inclination. Distortions of this shape may be secondary to heredity, aging, paralysis, trauma or previous surgery. This distortion of shape inevitably manifests as rounding of the fissure with inferomedial descent of the lateral canthus and concomitant descent of the lower lid margin. Lateral canthopexy, the surgical repositioning of the lateral canthus is fundamental to altering or restoring the shape of the palpebral fissure.
The lateral canthal structures are purchased with a figure of eight suture. Drill holes are placed in the lateral orbital rim using the zygomaticofrontal sutures as reference landmarks. This measured placement aids in achieving symmetric canthal repositioning. The bridge of bone between the drill holes provides a stable platform over which the suture ends can be tied.
Infraorbital Rim Augmentation
The relationship of the globe to the infra orbital rim is a primary determinant of the appearance of the upper portion of the midface. In young healthy Caucasian adults, the average projection of the soft tissues overlying the supraorbital rim beyond the surface of the cornea is about 10 mm, and the projection of the beyond the soft tissues overlying the infraorbital rim is 3 mm.
A lack of midface skeleton projection results in a deficiency for the support of the soft tissue envelope. Clinical manifestations include decent of the lower lid with a tendency for scleral show and a long lid and cheek sag. With this lack of skeletal support for the lower lid, aesthetic blepharoplasty is prone to lower lid malposition. This anatomy was termed as “morphologically prone” to lid descent after blepharoplasty by plastic surgeons Rees and La Trenta. Jelks and Jelks later referred to average globe-lower rim relation as a positive vector. A deficient infraorbital rim was termed a negative vector. Dr. Yaremchuk Designed infraorbital rim implants to “Reverse” the negative vector.
Lid malposition after lower lid blepharoplasty can be corrected by freeing periorbital scarring, augmenting the infraorbital rim with an infraorbital rim implant and elevating the midface tissues in the subperiosteal plane.
Clinical Examples Using These Techniques
This patient was referred with lid retraction from scarring after lower lid blepharoplasty and attempts for correction with a tarsal strip lid tightening. The lid retraction was corrected with a palatal spacer graft.


This patient had suffered massive right sided orbital trauma with loss of her globe. The orbital structures were reconstructed. However, the lower lid was insufficient to cover the orbital prosthesis. A conchal cartilage spacer graft and lower lid shortening provided lid support and prosthesis coverage and position stability.


This patient had lid descent after lower lid blepharoplasty with tarsal strip in negative vector patient. Surgery required Infraorbital rim augmentation, subperiosteal midface lift and palatal spacer grafts.


This patient was involved in an MVA and had orbital fractures the patient suffered a post-op infection resulting in the obvious lid malposition. Surgery was corrected with a palatal spacer graft to restore preinjury lower lid symmetry.

This patient with Graves Ophthalmopathy had her lower lids elevated with a palatal spacer graft.


This patient with Treacher-Collins Syndrome was left with lower lid distortion after reconstructive surgery. Lower lid shape and reconstruction involved augmentation of the infraorbital rim, a subperiosteal midface lift and a bridge-of bone lateral canthopexy.

This patient had an aggressive lower lid blepharoplasty resulting in lower lid descent. It was corrected by scar release and subperiosteal midface lift.

These two patients had agressive lower lid blepharoplasties resulting in lower lid descent. It was corrected by scar release, subperiosteal midface lift and lateral canthopexy.


Procedure Videos
* Reviews
*
"The message on the pen says it all. Thank you for being you, for being dedicated, sympathetic to my worries, for being brave and bold as a surgeon, and yet being impeccably gentle with your work. You helped me feel whole again. Indebted to you Sir. May God Bless you and your family from here to forever. With much respect and love."
-Sara
* "Honestly Dr. Yaremchuk has drastically changed my life forever. When I first came to him for my rhinoplasty consult I was on constantly the verge of tears about my appearance. I had a previous surgery from a different surgeon that had left me disfigured in my eyes. I went from having a small bump on the ridge of my nose to having my nose completely sideways post opt. I came to Dr. Yaremchuk in hopes that he could correct or even just partially correct my nose. Not only did he deliver, he exceeded all my expectations! He gave me back the nose I was born with (even a little cuter!) I HIGHLY recommend Dr. Yaremchuk and his staff to anyone looking for superior results. - Stephanie Poirier"
* "Everybody tells me that even after 2 years I have the best facelift they have ever seen. I know many of my friends and acquaintances have gone to see you. I hope some have actually gone ahead with the surgery. It makes such a difference in one's life."
* "I had an informal high school reunion recently, and though no one noticed the surgery, I felt some of my friends were, somehow, in "awe" of me. I felt they treated me better than before, and they respected me more. I felt like a real leader. I notice [second patient] is now more confidant, too. She has enjoyed shopping for new clothes to fit her new and improved physique. Her eyelid and nose look more natural and her chin more feminine. We thank you."
* "It's been a little over a month since my surgery and I'm just writing to say thank you very much for all the hard work you've done for me so many times already! I can only imagine how difficult it is trying to fix something that already turned into solid scarring instead of normal tissues after too many surgeries! I really don't know what would've happened to my face if I didn't find you!"
- This patient received revisional cosmetic surgery from Dr. Yaremchuk to correct deformities created during previous experiences with other plastic surgeons
* "I am so pleased with the results. The swelling has gone down alot. And I really look so good. And I know it will get even better with time. I still don't look exactly Iike I did before any surgery, but I did not expect that because of the previous operations. My forehead is still slightly higher than before. But I am very happy with what you could do. Thank you. The Lord has blessed you with a great skill to help people."
"It has been about a month since I stopped by for a Mandible Implant and my recovery has gone very well. The swelling and soreness went away weeks ago and I am back to exercising again. I'm really happy with the work you did and the great care of your staff."
- This patient underwent mandible implant surgery
* "I just wanted to thank you very, very much for the incredible results I already see from my surgery last week... The results look so natural. I'm so happy!"
* "I can say this with confidence: Dr. Yaremchuk saved my life. He saved the quality of my life... if you need plastic surgery, you can't do better than Dr. Michael J. Yaremchuk."
"...Watching you move confidently and even a bit excited toward a solution for my very challenged case, well it was almost [as] exciting for me too! Your talent and your attention to my case is something that warrants a note, a huge thanks, a big hug, applause and so much more.... My gratitude always."
"I just wanted to take this opportunity to tell you how thrilled I am with the results of my chin reduction surgery! Thrilled beyond measure. My only regret is not having found you years sooner. You are every bit as brilliant and talented as your reputation suggests."
"Thanks again for the great work, it's changed my life. I'll see you in a couple of years!"
* "I look better now then I ever did in my life even when I was in my twenties before I ruined my face.... I love the shape of my eyes, I couldn't wish for better, I look so pretty! You are and absolutely unique craftsmen doctor! I don't think there is anyone as talented as you are and it was nice to see that you are passing your experience to young surgeons, they are so lucky to learn from you! All the best to you from a very happy girl"
* "I will be forever grateful for everything you have done for me. You have changed my life!"
* "I know I'll have much more to thank you for as my recovery progresses - but I want to thank you now for doing my surgery and to tell you how much I appreciate your expertise and care. I felt I was in good hands and therefore was not too nervous. I'm grateful and very much appreciate your kindness in fixing my deviated septum along with my other nose imbalances. Your staff have been very helpful as well. Marge is incredibly pleasant to talk with by phone and the office staff and nurses have been very nice and quick to answer questions and concerns. Jan, who I consider "my" nurse, is sweet, efficient and attentive. Mary was great too as was the anesthesiologist who smoothly kept me in 'la la land' while you worked your magic."
- This patient underwent rhinoplasty surgery
* "I'm absolutely delighted with the outcome. Not just because the changes have made a vast improvement to my looks, but that not a single person has ever questioned me regarding PS. I could never have imagined my look could change so much, yet so discreetly. Fantastic.
I can't believe how great my eyes feel. I always thought I had allergies and that was why they hurt and burned so much. I am thrilled! The best part is not only do they feel great they look great too! Thank you Dr, Yaremchuk. The whole experience was wonderful. You have a great staff as well. As for the lip injection I would appreciate your discerning eye. If you feel i shouldn't
trust your judgement as i did when you recommended not doing the ULB. You are truly an artist."
* "It is as much a blessing as a relief to have you as my surgeon. Your peerless skill is matched only by your immense kindness and compassion. Thank you or all you do for me and for countless others. You have clearly devoted your entire life to our care, and we are all the better for it."
* "I have been meaning to write to you to tell you again how happy I have been with the brilliant work you did on my chin and jaw. I have been utterly thrilled ever since I was able to see the final results... You really are a genius. The combination of being an artist and a doctor is quite an impressive gift..."
-This patient underwent cosmetic surgery of the chin and jaw
"... I'm looking way better and I'm really happy and grateful for all amazing work you did for me!... you are an amazing artist and I trust you with my face and my life. Lots of love, and my best wishes to you and your fantastic team!"
"I just want to thank you so much for what you have done for me. You really are the best in your field."
* "There really is no way for me to adequately explain the feeling of incredible gratitude I have for your help last week... I shall always remember the compassionate assistance you showed me."
* "I, unfortunately, have had a couple awful encounters with plastic surgery. Borderline disasters. Dr. Y has tactics in solving problems that other doctors don't. I had an under the eye problem and the only solution I thought there was was cheek implants. Instead with his orbital rim implant he fixed the problem perfectly. I had been self conscious about my looks my entire life and now I am no longer... He was kind to me and to my father and his staff are sweet people as well... [H]e's just a good guy who happens to be the best at what he does. I'm beyond sastified and will never have to experience a painful cosmetic operation again thanks to him. My life is changed."
-This patient received revisional cosmetic surgery
* "I know you said I'd get the final results in about 3 months, but I'm already ecstatic at the results. My only regret is that I didn't do this 5 years ago."
* "In terms of surgical skill and experience, Dr. Yaremchuk is pretty much as good as it gets. I can happily put my full weight behind this review to say that I unequivocally recommend him to anyone looking for facial skeletal changes.
You can also review his literature contributions online and see that he is the leader in the field. In fact, I doubt anyone out there even comes close.
Beyond the surgical elements, his response times, willingness to engage, empathy, and overall bedside manner are great. True intent always shines through, and you can see that he really is in it for the patients - i.e., he's passionate about putting his patients first and taking on difficult cases to get people the result they're looking for
"
* "It's unbelievable that a just a few millimeters along the mandible could make such a huge difference -- but they have. I don't even think about the implants anymore, they are just a part of my native face. I feel like this is how I was supposed to look, the best version of me. My only regret is that I didn't do this earlier. "