* Reviews
*
"The message on the pen says it all. Thank you for being you, for being dedicated, sympathetic to my worries, for being brave and bold as a surgeon, and yet being impeccably gentle with your work. You helped me feel whole again. Indebted to you Sir. May God Bless you and your family from here to forever. With much respect and love."
-Sara
* "Honestly Dr. Yaremchuk has drastically changed my life forever. When I first came to him for my rhinoplasty consult I was on constantly the verge of tears about my appearance. I had a previous surgery from a different surgeon that had left me disfigured in my eyes. I went from having a small bump on the ridge of my nose to having my nose completely sideways post opt. I came to Dr. Yaremchuk in hopes that he could correct or even just partially correct my nose. Not only did he deliver, he exceeded all my expectations! He gave me back the nose I was born with (even a little cuter!) I HIGHLY recommend Dr. Yaremchuk and his staff to anyone looking for superior results. - Stephanie Poirier"
* "Everybody tells me that even after 2 years I have the best facelift they have ever seen. I know many of my friends and acquaintances have gone to see you. I hope some have actually gone ahead with the surgery. It makes such a difference in one's life."
* "I had an informal high school reunion recently, and though no one noticed the surgery, I felt some of my friends were, somehow, in "awe" of me. I felt they treated me better than before, and they respected me more. I felt like a real leader. I notice [second patient] is now more confidant, too. She has enjoyed shopping for new clothes to fit her new and improved physique. Her eyelid and nose look more natural and her chin more feminine. We thank you."
* "It's been a little over a month since my surgery and I'm just writing to say thank you very much for all the hard work you've done for me so many times already! I can only imagine how difficult it is trying to fix something that already turned into solid scarring instead of normal tissues after too many surgeries! I really don't know what would've happened to my face if I didn't find you!"
- This patient received revisional cosmetic surgery from Dr. Yaremchuk to correct deformities created during previous experiences with other plastic surgeons
* "I am so pleased with the results. The swelling has gone down alot. And I really look so good. And I know it will get even better with time. I still don't look exactly Iike I did before any surgery, but I did not expect that because of the previous operations. My forehead is still slightly higher than before. But I am very happy with what you could do. Thank you. The Lord has blessed you with a great skill to help people."
"It has been about a month since I stopped by for a Mandible Implant and my recovery has gone very well. The swelling and soreness went away weeks ago and I am back to exercising again. I'm really happy with the work you did and the great care of your staff."
- This patient underwent mandible implant surgery
* "I just wanted to thank you very, very much for the incredible results I already see from my surgery last week... The results look so natural. I'm so happy!"
* "I can say this with confidence: Dr. Yaremchuk saved my life. He saved the quality of my life... if you need plastic surgery, you can't do better than Dr. Michael J. Yaremchuk."
"...Watching you move confidently and even a bit excited toward a solution for my very challenged case, well it was almost [as] exciting for me too! Your talent and your attention to my case is something that warrants a note, a huge thanks, a big hug, applause and so much more.... My gratitude always."
"I just wanted to take this opportunity to tell you how thrilled I am with the results of my chin reduction surgery! Thrilled beyond measure. My only regret is not having found you years sooner. You are every bit as brilliant and talented as your reputation suggests."
"Thanks again for the great work, it's changed my life. I'll see you in a couple of years!"
* "I look better now then I ever did in my life even when I was in my twenties before I ruined my face.... I love the shape of my eyes, I couldn't wish for better, I look so pretty! You are and absolutely unique craftsmen doctor! I don't think there is anyone as talented as you are and it was nice to see that you are passing your experience to young surgeons, they are so lucky to learn from you! All the best to you from a very happy girl"
* "I will be forever grateful for everything you have done for me. You have changed my life!"
* "I know I'll have much more to thank you for as my recovery progresses - but I want to thank you now for doing my surgery and to tell you how much I appreciate your expertise and care. I felt I was in good hands and therefore was not too nervous. I'm grateful and very much appreciate your kindness in fixing my deviated septum along with my other nose imbalances. Your staff have been very helpful as well. Marge is incredibly pleasant to talk with by phone and the office staff and nurses have been very nice and quick to answer questions and concerns. Jan, who I consider "my" nurse, is sweet, efficient and attentive. Mary was great too as was the anesthesiologist who smoothly kept me in 'la la land' while you worked your magic."
- This patient underwent rhinoplasty surgery
* "I'm absolutely delighted with the outcome. Not just because the changes have made a vast improvement to my looks, but that not a single person has ever questioned me regarding PS. I could never have imagined my look could change so much, yet so discreetly. Fantastic.
I can't believe how great my eyes feel. I always thought I had allergies and that was why they hurt and burned so much. I am thrilled! The best part is not only do they feel great they look great too! Thank you Dr, Yaremchuk. The whole experience was wonderful. You have a great staff as well. As for the lip injection I would appreciate your discerning eye. If you feel i shouldn't
trust your judgement as i did when you recommended not doing the ULB. You are truly an artist."
* "It is as much a blessing as a relief to have you as my surgeon. Your peerless skill is matched only by your immense kindness and compassion. Thank you or all you do for me and for countless others. You have clearly devoted your entire life to our care, and we are all the better for it."
* "I have been meaning to write to you to tell you again how happy I have been with the brilliant work you did on my chin and jaw. I have been utterly thrilled ever since I was able to see the final results... You really are a genius. The combination of being an artist and a doctor is quite an impressive gift..."
-This patient underwent cosmetic surgery of the chin and jaw
"... I'm looking way better and I'm really happy and grateful for all amazing work you did for me!... you are an amazing artist and I trust you with my face and my life. Lots of love, and my best wishes to you and your fantastic team!"
"I just want to thank you so much for what you have done for me. You really are the best in your field."
* "There really is no way for me to adequately explain the feeling of incredible gratitude I have for your help last week... I shall always remember the compassionate assistance you showed me."
* "I, unfortunately, have had a couple awful encounters with plastic surgery. Borderline disasters. Dr. Y has tactics in solving problems that other doctors don't. I had an under the eye problem and the only solution I thought there was was cheek implants. Instead with his orbital rim implant he fixed the problem perfectly. I had been self conscious about my looks my entire life and now I am no longer... He was kind to me and to my father and his staff are sweet people as well... [H]e's just a good guy who happens to be the best at what he does. I'm beyond sastified and will never have to experience a painful cosmetic operation again thanks to him. My life is changed."
-This patient received revisional cosmetic surgery
* "I know you said I'd get the final results in about 3 months, but I'm already ecstatic at the results. My only regret is that I didn't do this 5 years ago."
* "In terms of surgical skill and experience, Dr. Yaremchuk is pretty much as good as it gets. I can happily put my full weight behind this review to say that I unequivocally recommend him to anyone looking for facial skeletal changes.
You can also review his literature contributions online and see that he is the leader in the field. In fact, I doubt anyone out there even comes close.
Beyond the surgical elements, his response times, willingness to engage, empathy, and overall bedside manner are great. True intent always shines through, and you can see that he really is in it for the patients - i.e., he's passionate about putting his patients first and taking on difficult cases to get people the result they're looking for
"
* "It's unbelievable that a just a few millimeters along the mandible could make such a huge difference -- but they have. I don't even think about the implants anymore, they are just a part of my native face. I feel like this is how I was supposed to look, the best version of me. My only regret is that I didn't do this earlier. "
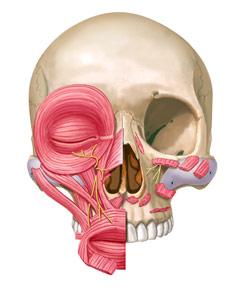
Malar (Cheek) Implants
The malar area is the most projecting part of the midface skeleton. It is what we consider the "cheekbone." Prominent malar bones are considered attractive. Hence, the malar area is frequently augmented with implants. Oftentimes, a deficiency in cheek prominence is part of a more generalized deficiency in the midface skeleton. For that reason, malar (cheek) implants are often used in combination with other implants - most frequently, with infraorbital rim implants, which build up the area directly beneath the eye.
Patients who have had malar implant surgery are shown to the right. Note the elevated and more attractive and youthful position of the cheek prominence in each of these patients.
 Click here to
see revisional surgery/malar implant patient examples, which Dr. Yaremchuk corrected.
Click here to
see revisional surgery/malar implant patient examples, which Dr. Yaremchuk corrected.
Dr. Yaremchuk was interviewed for Harper’s Bazaar on cheek implants. To read the article, click here
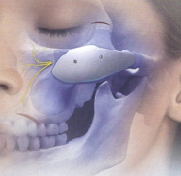
This figure shows a typical position and shape of a malar implant:
Dr. Yaremchuk’s thoughts on and the nuances of malar implant surgery
It has been challenging for researchers and surgeons alike to gather measurements describing the average malar area across people of varying age, sex, and ethnicity because it is a dome-like shape with an absence of easily defined landmarks that are projected to the surface of the skin. Several landmarks lie adjacent to, or involve portions of the malar bone, but there are none defining an area of maximum malar prominence. The resultant paucity of objective data describing the malar area has inevitably made implant augmentation of this area more subjective. Because it is difficult to define what is average or normal for the malar area, selection of implant shape, implant size and implant position for malar augmentation can be problematic.
Several surgeons, working without quantitative data, have suggested techniques to identify the malar prominence as a guide to malar augmentation. Their techniques use fixed relations to various anatomic landmarks to determine an ideal position of malar prominence.
The lack of consensus regarding the most projecting point of the malar prominence reflects the plastic surgeon’s dilemma.
After analyzing many attractive faces, three dimensional facial CT scans and anatomic specimens, I have concluded that the most projecting part of the malar area bone is relatively high – “high and near the eye”. I have found that the point intersecting a vertical line through the lateral canthus with a horizontal line through the infraorbital foramen to be a useful reference point when positioning or designing malar implants.
As the most prominent and surgically accessible portion of the midface and, until recently, the only area of the midface for which implants were available, many patients receive malar implants when the entire midface or another midface area is deficient. This may exaggerate the facial imbalance. For example, malar augmentation, particularly when it extends far onto the zygomatic arch, may exaggerate the appearance of prominent eyes due to midface hypoplasia. These patients are better served with augmentation of the infraorbital rim alone or, in combination with malar augmentation and other soft tissue manipulations.
Since full cheeks are associated with youth, malar augmentation is often performed to provide a youthful appearance. This may provide an aesthetic benefit if there is a relative malar hypoplasia or if the implants are of modest size and projection. This skeletal augmentation is not equivalent to a soft tissue augmentation or resuspension. Similarly, malar implants are often advocated as a means to obliterate lower eyelid wrinkles or secondary bags. Malar augmentation typically does not correct these surface irregularities, however. More often, they detract from periorbital aesthetics by contributing to lower lid malposition, particularly when placed through an eyelid approach.
Certain implant designs do not mimic the contours of the midface skeleton. For example, submalar implants are designed to be placed over and below the origin of the masseter muscle - a location where there is no midface skeleton - in an attempt to provide cheek fullness. It is often performed as an adjunct to, or as an alternative to a facelift. The result is an unnatural midface – one with too much lower midface fullness which actually detracts from malar definition and projection.
In summary, the lack of anthropometric and cephalometric landmarks precludes the availability of normative data making analysis and augmentation of the malar area largely subjective. As a result, malar implants are often misused to address issues better corrected through other techniques. Malar deficiency is often part of a generalized midface deficiency for which malar augmentation alone may be inadequate or, even, inappropriate. Clinical experience has shown that when malar projection is deemed inadequate, malar augmentation is most effective when it recreates the contours of a normal skeleton with prominent anterior projection.
This figure shows a typical position and shape of a malar implant

