Correcting Post Orthognathic Surgery Irregularities
Le Fort I osteotomy with advancement and sagittal split osteotomy of the mandible may be performed alone or in combination to correct occlusal disharmony and to improve appearance. Sliding genioplasty is often performed alone or in combination with sagittal split osteotomy. These procedures may leave certain patients with characteristic contour irregularities.
Patients who undergo Le Fort I advancement are often left with residual deficiency in their upper midface (the area between their eyes and the osteotomy). The result is an exaggerated fullness in the lower midface. This is a look distinctly different from the upper cheek fullness seen in the attractive youthful face. This imbalance of facial proportion can be corrected by augmenting the area beneath the eye (infraorbital rim augmentation) and resuspending the cheek soft tissues (midface lift).
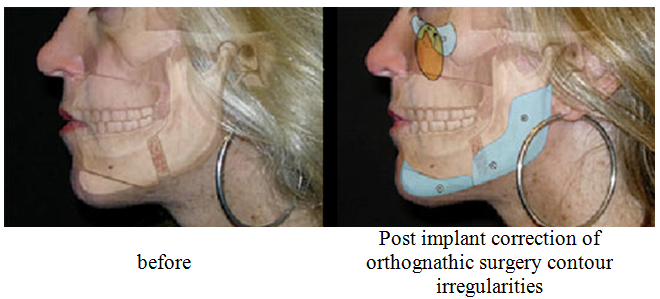
The figure below shows a patient who has had a Le Fort I advancement, sagittal split osteotomy,and sliding genioplasty resulting in contour imbalance and irregularities. The artist has rendered the underlying skeletal contour responsible for the appearance on the left and, on the right, the surgical correction accomplished with strategically placed infraorbital rim, posterior mandible and chin implants, as well as midface and chin soft tissue resuspensions.
Sagittal split osteotomy of the mandible separates the tooth bearing symphysis and adjacent bodies from the non tooth-bearing but articulating rami. Requisites for positioning the resultant anterior and posterior segments to improve occlusion, allow bone healing, and continue joint function may result in displeasing postoperative contour. The advancement of the distal, or tooth bearing, segment is dictated by occlusal relations. It inevitably creates a contour irregularity at the site of the body osteotomy and distal segment advancement. This area of narrowing may be visible, and even disfiguring, in certain individuals. Positioning of the posterior segment requires that the condyle be seated in the glenoid fossa and that there be sufficient segment contact to allow bone healing. Fulfillment of these requisites dictates the position of the ramus and its angle. This may result in an aesthetically displeasing position of the ramus angle with insufficient height, insufficient width, or asymmetry. Mandible implants can be used to improve contour in these patients.
The figure below shows a patient who has had a sagittal split osteotomy,and sliding genioplasty resulting in contour imbalance and irregularities. The artist has rendered the underlying skeletal contour responsible for the appearance on the left and, on the right, the surgical correction accomplished with strategically placed posterior mandible and chin implants.

Sliding genioplasty is often performed alone or in combination with sagittal split osteotomy. Sliding genioplasty involves a horizontal osteotomy of the mandible just beneath the mental foramen. A now freed chin point is positioned as desired, usually anteriorly to increase chin projection, but theoretically, can be moved any direction. Sliding genioplasty may result in an unnatural body and border contour that accompanies the selective movement of the chin point. The contour that results is one that has a poor transition resulting in a stuck on appearance of the chin as well as a step-off at the site of osteotomy along the mandibular body. The notching or indentation is especially detrimental to those who have a pre existing pre-jowl sulcus. Appropriately placed implants can correct these contour deformities.