170 Commonwealth Avenue, Suite 101 Boston, MA 02116
Phone: (617) 726-5280
Aging of the Facial Skeleton: Aesthetic Implications and Rejuvenation Strategies
Background: Facial aging is a dynamic process involving the aging of soft-tissue and bony structures. In this study, the authors demonstrate how the facial skeleton changes with age in both male and female subjects and what impact these structural changes may have on overall facial aesthetics.
Methods: Facial bone computed tomographic scans were obtained from 60 female and 60 male Caucasian subjects. Twenty male and 20 female subjects were placed in three age categories (20 to 40 years, 41 to 64 years, and 65 years and older). Each computed tomographic scan underwent three-dimensional reconstruction with volume rendering. Edentulous patients were excluded. The following measurements were obtained: upper face (orbital aperture area, orbital aperture width, and curvilinear analysis of the superior and inferior orbital rims), midlface (glabellar angle, pyriform angle, maxillary angle, and pyriform aperture area), and lower face (bigonial width, ramus breadth, ramus height, mandibular body height, mandibular body length, and mandibular angle). Results: The orbital aperture width and orbital aperture area increased significantly with age for both sexes. There was a significant increase in orbital aperture size (increase in height of the superomedial and inferolateral orbital rim) in both sexes. The glabellar and maxillary angles decreased significantly with age for both sexes, whereas the pyriform aperture area significantly increased for both sexes with age. Mandibular length and height both decreased significantly for each sex. The mandibular angle significantly increased with age for both sexes.
Conclusions:
These results suggest that the skeletal morphology of the face changes with age. This change in skeletal morphology may contribute to the appearance of the aging face. (Plast. Reconstr. Surg. 127: 374, 2011.)
To effectively rejuvenate the aging face, it is necessary to understand the dynamic aging process. Epidermal thinning and the decrease in collagen cause skin to lose its elasticity. Loss of fat, coupled with gravity and muscle pull, leads to wrinkling and the formation of dynamic lines. These factors contribute to the formation of nasolabial folds, jowls, crow’s feet, and the sagging appearance of aged facial skin.
The aging process has also been shown to affect the facial bones. Multiple studies suggest that the bony aging of the orbit and midface is a process primarily of contraction and morphologic change.
From the Divisions of Plastic and Reconstructive Surgery, Departments of General Surgety of University of Rochester Medical Center, Stanford University Medical Center, and Harvard University Medical Center.
Received for publication April 17, 2010; accepted July 19, 2010.
Copyright ©2010 by the American Society of Plastic Surgeons DOI: 10.1097/PRS.0b013e3181f95b2d
1-7 Past studies by our group analyzing the midface and orbit in smaller sample sizes found that the facial bones experience volume loss with increasing age. In this study, we incorporate and expand on all our previous work and present the aging of the face in its entirety and in a substantially larger subject size. We also explore the aesthetic implications of these structural changes and provide possible rejuvenation strategies for each area of the face.
SUBJECTS AND METHODS
Computed tomographic scans of the facial bones, at a slice width of 1.0 mm, were obtained from 120 Caucasian subjects (60 women and 60 men). There were 20 male and 20 female subjects in each of three age categories: young (20 to 40 years), middle (41 to 64 years), and old (65 years or older). Subjects underwent computed tomographic scanning for the following medical reasons: to rule out facial bone fracture (n = 75), to assess severe sinusitis (n = 28), and for a soft-tissue diagnosis (cellulitis, soft-tissue mass, or to rule out abscess) ( n =17). Only scans negative for fracture and without signs of past fracture or bony involvement, in cases of soft-tissue disease, were included in this study. Edentulous patients were excluded from this study.
Each computed tomographic scan underwent volume-rendered three-dimensional reconstruction using the three-dimensional analysis software Volume Viewer (Voxtool 3.0.64q; GE Healthcare, Bucks, United Kingdom). Each model was stabilized in the standard anterior cranial base position of sella nasion. The following measurements were then taken.
Orbit
The orbital aperture area, orbital aperture width (distance from the posterior lacrimal crest to the fron to zygomatic suture), and curvilinear analysis of the superior and inferior orbital rim (distance from the orbital width axis to the superior orbital rim and inferior orbital rim at nine equal increments [referred to as x coordinates 10 to 90 (Fig. 1)] were obtained.
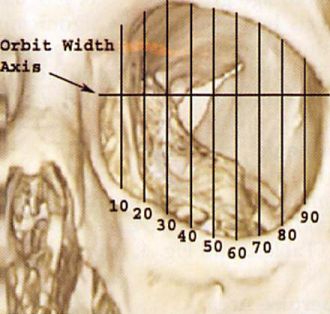
Fig.1. The distance from the orbital width axis to the superior and inferior orbital rims was obtained at nine equal increments.
Midface
The glabellar angle (maximal prominence of the glabella to the nasofrontal suture), pyriform angle (nasal bone to lateral inferior pyriform aperture) , maxillary angle (superior to inferior maxilla at the articulation of the inferior maxillary wing and alveolar arch), and pyriform aperture area were obtained. Each angle was taken in reference to the sella-nasion line.
Mandible
The bigonial width (distance between the right and left gonion), ramus breadth (minimum breadth of the mandibular ramus), ramus height (distance from the mandibular condyle to the gonion), mandibular body height (distance from the infradentale to the gnathion), mandibular body length (anterior margin of the chin to a center point on the projected straight line placed along the posterior border of the two mandibular angles), and mandibular angle (the angle formed by the inferior border of the mandibular body and the posterior border of the ramus) were obtained (Figs. 2 and 3).

Fig. 2. 7, Bigonial width (distance between the right and left gonion); 2, mandibular body height (distance from the infradenÂtale to the gnathion) (go, gonion; gn, gnathion).
All measurements were made on a General Electric Advantage Windows workstation (General Electric Co., Waukesha, Wis.), running version 4.2 software on HP xw8000s (Hewlett-Packard Company, Palo Alto, Calif.). One-way analysis of variance was used to analyze results within each sex across age groups. Results were considered significant at a value of p < 0.05.
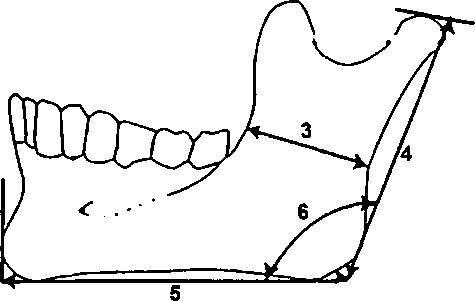
Fig. 3. 3, Ramus breadth (breadth of the mandibular ramus at the narrowest point); 4, ramus height (distance from the highest point on the mandibular condyle to the gonion); 5, mandibular body length (anterior margin of the chin to the gonion); 6, mandibular angle (the angle formed by the inferior border of the manÂdibular body and the posterior border of the ramus).
RESULTS
The mean age in the young age group was 26.3 years for our male subjects and 24.7 years for our female subjects. The male subjects in our middle age group had a mean age of 51.3 years, whereas the female subjects had a mean age of 50.2 years. The mean age in the old age group was 76 years for our male subjects and 81.1 years for our female subjects (Table 1).
| Table 1. Average Age by Sex in Each Age Category |
| Young (yr) | Middle (yr) | Old (yr) | |||
| Male Female | Male | Female | Male | Female | |
| Mean
Range SD |
26.3 24.7 20-31 20-36 3.9 5.4 | 51.3
41-61 8.5 |
50.2
41-64 7.3 |
76
66-86 6.5 |
81.1
65-93 8.4 |
Orbit
Orbital Aperture Width
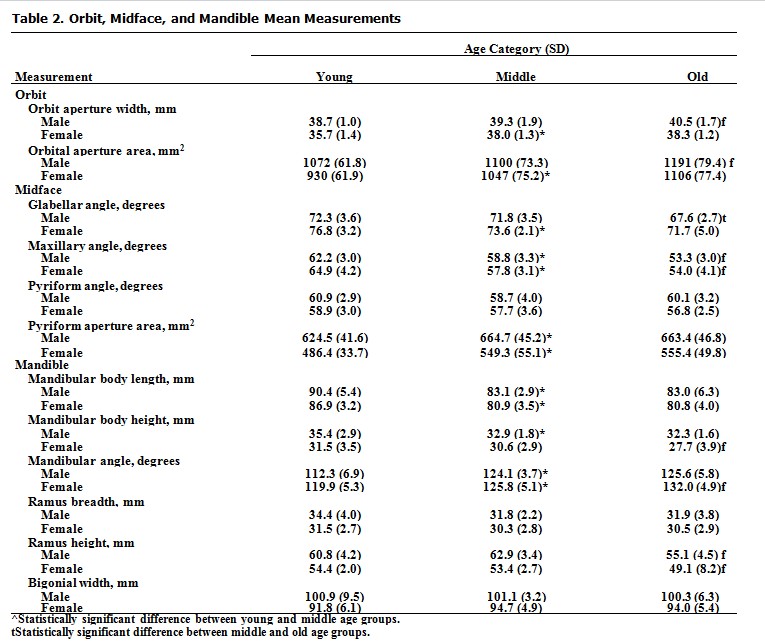
The orbital aperture width increased significantly with age for both male (F = 6.012, p = 0.0043) and female {F— 24.81, p < 0.0001) study populations. Male subjects had a statistically significant increase from the young age group to the old age group (t = 3.4, p Orbital Aperture Area
The orbital aperture area increased significantly with age for both male (F = 15.03, p < 0.0001) and female (F= 31.16, p < 0.0001) study populations. Male subjects had a statistically sig-nificant increase from the middle age group to the old age group (t = 5.2, p < 0.05). Female subjects had a statistically significant increase from the young age group to the middle age group (t = 5.17, p < 0.01) (Table 2 and Fig. 4, below).
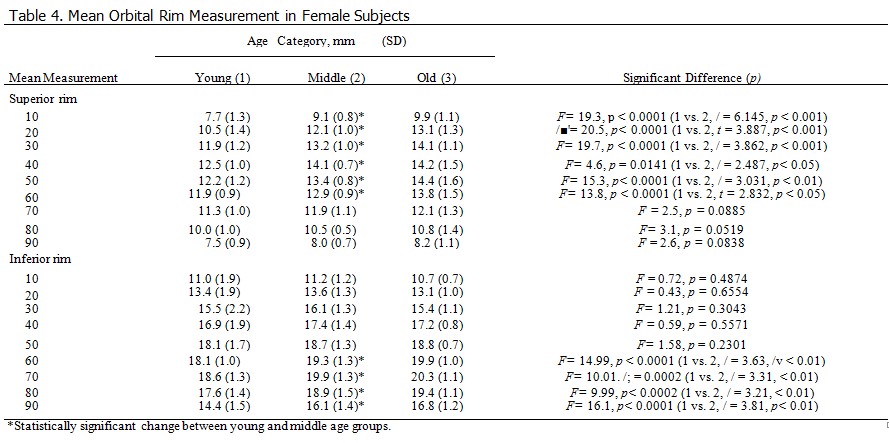
Superior Orbital Rim
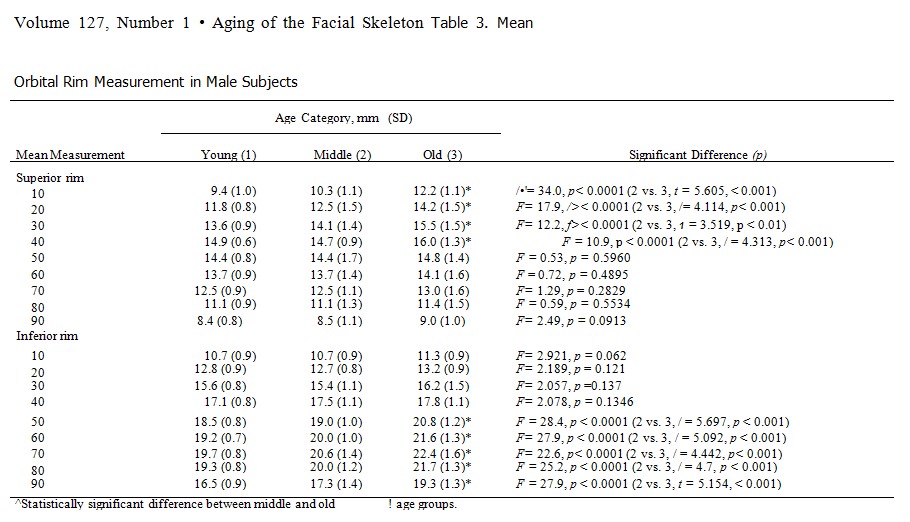
There was a significant increase in the distance to the superior orbital rim from * coordinates 10 to 40 for our male subjects (Table 3) and from x coordinates 10 to 60 for our female subjects (Table 4). This change occurred between the young and middle age groups for our female subjects and between the middle and old age groups for our male subjects.
Inferior Orbital Rim
There was a significant increase in the distance to the inferior orbital rim from x coordinates 60 to 90 for our female population subjects (Table 4) and from x coordinates 50 to 90 for our male subjects (Table 3). Again, this change occurred between the young and middle age groups for our female subjects and between the middle and old age groups for our male subjects.
Midface
Glabellar Angle
The glabellar angle decreased significantly with age for both male (F= 12.29, p< 0.0001) and female (F= 9.99, p = 0.0002) study populations. Male subjects had a statistically significant de-crease from the middle age group to the old age group (t = 4.2, p < 0.001). Female subjects had a statistically significant decrease from the young age group to the middle age group (t = 2.7, p < 0.05) (Table 2 and Fig. 4).
Maxillary Angle
The maxillary angle decreased significantly with age for both male (F= 42.01, p < 0.0001) and female {F= 40.95, p < 0.0001) study populations. Male subjects had a statistically significant decrease from the young age group to the middle age group (t = 3.4, p < 0.01) and from the middle age group to the old age group (t = 5.6, p < 0.001). Female subjects had a statistically significant decrease from the young age group to the middle age group {t = 5.8, p < 0.001) and from the middle age group to the old age group (J = 3.1, p < 0.01) (Table 2 and Fig. 4, below).
Pyriform Angle
The pyriform angle showed no significant change with increasing age for both male (F= 2.163, p— 0.1243) and female (F= 2.M,p= 0.1047) study populations (Table 2 and Fig. 4, below).
Pyriform Aperture Area
The pyriform aperture area increased significantly with increasing age for both male (F= 5.26, p = 0.008) and female (F = 13.16, p < 0.0001) study populations. Male subjects had a statistically significant increase from the young age group to the middle age group (t = 2.85, p < 0.05). Female subjects had a statistically significant increase from the young age group to the middle age group {t = 4.22, p < 0.01) (Table 2 and Fig. 4,below)
Mandible
Bigonial Width and Ramus Breadth
Bigonial width did not change significantly with increasing age for either male (F = 0.09, p = 0.91) or female subjects (F = 1.36, p = 0.26) (Table 2 and Fig. 5, below).
Ramus breadth did not change significantly with increasing age for either male (F= 2.5 p —0.056) or female subjects (F = 0.88, p = 0.42) (Table 2 and Fig. 5, below).
Ramus Height
The ramus height decreased significantly with age for both male {F = 5.19, p < 0.0001) and female (F= 17.36, p< 0.0001) study populations. Male subjects had a statistically significant de-crease from the middle age group to the old age group (t = 5.77, p < 0.001). Female subjects had a statistically significant decrease from the middle age group to the old age group {t = 2.5, p < 0.05) (Table 2 and Fig. 5, below).
Mandibular Body Height
The mandibular body height decreased significantly with age for both male (F = 9.8, p = 0.0002) and female (F = 6.03, p = 0.0043) study populations. Male subjects had a statistically significant from the young age group to the middle age group (/ = 6.404, p < 0.001). Female subjects had a statistically significant increase from the young age group to the middle age group (1 = 3.38, p < 0.01) and between the middle age group and the old age group (/ = 3.87, p < 0.001) (Table 2 and Fig. 5).
Much is known with regard to the aging of the facial skin and subcutaneous tissues.8-10 This knowledge has made soft-tissue redraping and skin reduction the predominant approach for rejuvenating the aging face. Soft-tissue augmentation to replace volume loss has become more accepted recently by many to enhance the treatment plan for those seeking facial rejuvenation.11-13 This volume loss is likely caused by soft-tissue atrophy in addition to a loss of bony support and projection. The bony components of the face are important for overall facial three- dimensional contour, as they provide the framework on which the soft-tissue envelope drapes. If this framework experiences a morphologic change with age, the overlying soft tissues will subsequently project differently.
DISCUSSION
Soft-tissue fillers can be used successfully to restore volume loss caused by facial aging, particularly in the following anatomical regions: nasolabial fold, glabellar crease, malar region, nasojugal groove, and lips.14 As the majority of facial volume loss through aging is attributable to fat loss, fat may represent the ideal soft-tissue replacement.
Improvements in technique have enhanced the predictability of facial fat grafting. When autologous fat is not an option, alternative facial fillers including calcium hydroxylapatite and hyaluronic acid may provide excellent results.15
Skeletal augmentation, using implants made of silicone or porous polyethylene, is a simple and effective method of reversing age-related changes of the facial skeleton in patients with intact occlusion. Skeletal implants correct concave morphology. by increasing projection and provide a means of resuspending soft tissues that have descended off a deficient bony platform.1617 Silicone implants are a popular choice for skeletal reconstruction and augmentation and provide efficient and effective rejuvenation, especially with the use of the textured Silastic implant.18 The rates of extrusion and malposition of the silicone implants over time, however, have led some to use more porous textured implants. The clinical utility and morbidity associated with the use of porous polyethylene facial implants has been described well. Yaremchuk reported in 2003 on 370 consecutive implants with an average follow-up of 27 months. The overall reoperation rate was 10 percent (n = 16), which included operations to remove implants because of infections (n = 4) or to improve displeasing contours (n = 12).19 Skeletal augmentation offers a permanent rejuvenation of the facial skeleton and may be performed in conjunction with soft-tissue redraping. A discussion of our findings for each part of the face and possible aesthetic effects follows.
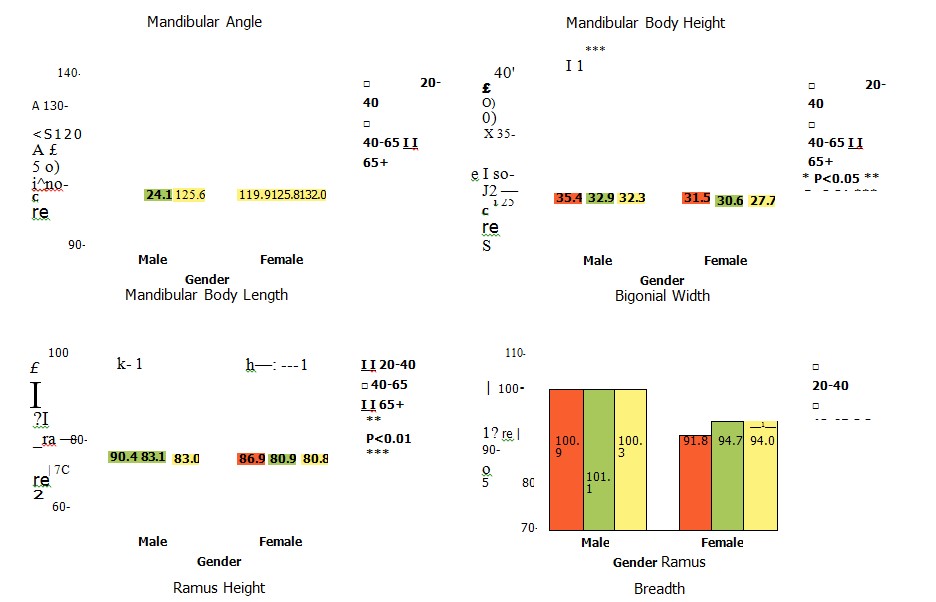
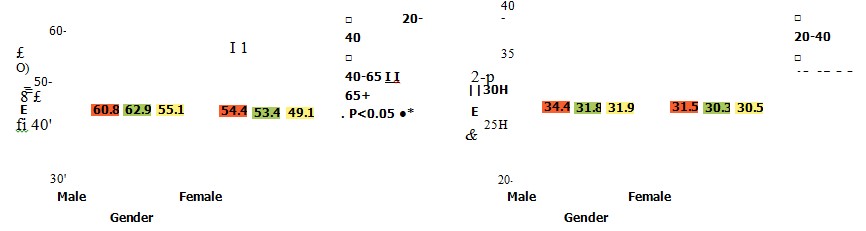
Fig. 5. Column graphs illustrating no statistically significant change in bigonial width or ramus breadth for either sex. Ramus height, mandibular body height, and mandibular body length showed a statistically significant decrease with age for both sexes. There was also a statistically significant increase in mandibular angle for both sexes with increasing age.
Orbit and Midface
Superomedial rim remodeling may contribute to the unmasking of the medial upper lid fat, a change currently attributed to weakening of the orbital septum. This in combination with the glabellar angle becoming more acute with age may also lead to the perceived descent of the medial brow and the formation of glabella skin creases. The inferolateral rim remodeling and increase in orbital aperture width may contribute to the formation of crow’s feet and lower lid lag (Fig. 6).
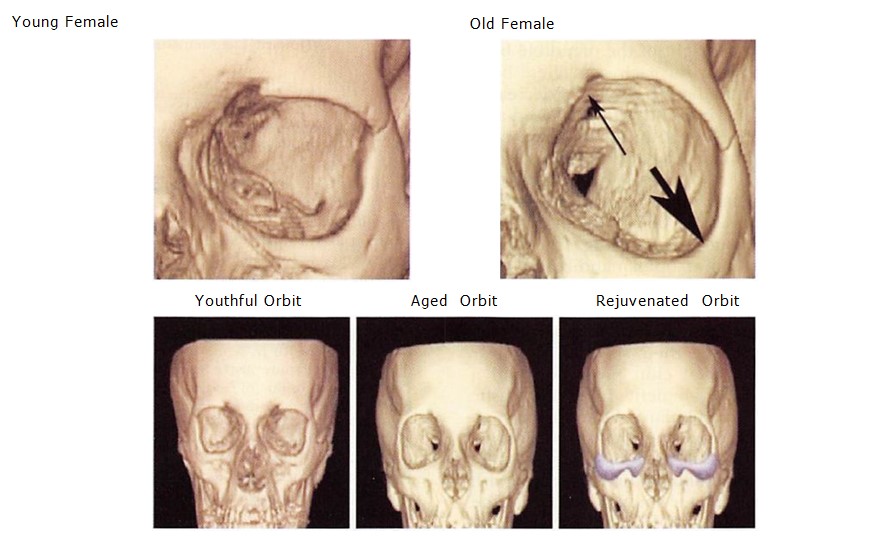
Fig. 6. (Above) Example images ofthe bony orbit of a young female subject on the left and an old female subject on the right (different subject). (Below) The aged orbit may be rejuve¬nated with volume augmentation.
381
As we try to further develop a concept of how the periorbital area changes with age, a possible working hypothesis is that the bony structures undergo morphologic change and also result in a widening of the orbital aperture that results in a change in the appearance of the overlying soft-tissue envelope. The overall widening of the orbital aperture results in a change in the relationship between the orbital contents and the surrounding bony framework. This may result in changes such as prominence of fat pads, deepening of sulci, or the enophthalmos and ptosis that may be seen with aging.
The changes seen in the upper half of the orbit may result in the soft tissues rolling into the orbital aperture and thus the appearance of brow descent and lateral orbital hooding. In the lower half of the orbit, the tissues may roll over the recessed bony ledge, leading to lag of the lower lid, prominence of lower lid fat pockets, and deepening of the nasojugal groove as disproportionate tissue piles up against the orbicularis origin along the medial rim and the origin of the orbicularis is reshaped with its underlying bony attachment. The decrease in maxillary angle may lead to decreased skeletal support for the malar fat pad, which may allow die nasolabial crease to become more prominent. The increase in pyriform aperture with increased age may contribute to decreased nasal support and projection.
Mandible
The length and height of the mandible both decreased significantly for each sex. These bony changes may result in the appearance of decreased chin projection that is found with increased age. The mandible is the foundation of the lower face, and any change in mandibular projection, width, or height can affect overall aesthetics. Patients with a normal mandibular ramus height and length of the mandibular body have an excellent support for soft-tissue repositioning. In contrast, those with a short ramus, open mandibular angle, and short mandibular body have poor skeletal support for midface and perioral soft-tissue repositioning and often benefit from volumetric augmentation to enhance their skeletal support.20 Patients with decreased chin projection and a prejowl sulcus often benefit from alloplastic augmentation.21 Mandibular volume loss also affects the aging of the neck, as it may contribute to the increased laxity of the platysma and soft tissues of the neck. The mandibular angle increased with age for both sexes in our study population. The increase in mandibular angle may result in blunting or the loss of definition of the lower border of the face. A blunted mandibular angle creates a loss of jawline definition (Fig. 7).
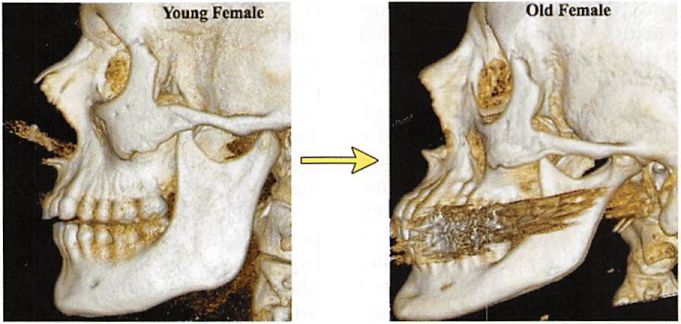 Fig. 7. Example images of the bony mandible of a young female subject on the left and an old female subject on the right (different subject).
Fig. 7. Example images of the bony mandible of a young female subject on the left and an old female subject on the right (different subject).
CONCLUSIONS
The facial skeleton experiences morphologic change and an overall decrease in volume with increasing age. This results in decreased support and projection of the soft-tissue envelope. This in addition to the decrease in facial fat leads to the appearance of the aged face. Howard N. Langstein, M.D. Division of Plastic Surgery University of Rochester Medical Center 601 Elmwood Avenue, Box 661 Rochester, N.Y. 14642 Howard_Langstein@urmc.rochester.edu
REFERENCES
1. Pessa JE, Chen Y. Curve analysis ofthe aging orbital aperture. Plast Reconslr Surg. 2002;109:751-755.
2. Zadoo VP, Pessa JE. Biological arches and changes to the curvilinear form of the aging maxilla. Plast Reconslr Surg. 2000;106:460-466.
3. Pessa JE, Zadoo VP, Mutimer KL, et al. Relative maxillary retrusion as a natural consequence of aging: Combining skeletal and soft tissue changes into an integrated model of midfacial aging. Plast Reconslr Surg. 1998 102:205-212.
4. Shaw RBJr, Kahn DM. Aging ofthe midface bony elements: A three dimensional CT study. Plast Reconslr Surg 2007;119: 675-681. Kahn DM, Shaw RB Jr. Aging of the bony orbit: A three dimensional CT study. Aesthet SurgJ. 2008;28:258-264.
5. Pessa JE. An algorithm of facial aging: Verification of Lam- bros’s theory by three-dimensional stereolithography, with reference to the pathogenesis of midfacial aging, scleral show, and the lateral suborbital trough deformity. Plast Re- const r Surg. 2000;106:479-487.
6. PessaJE, Zadoo VP, Yuan C, et al. Concertina effect and facial aging: Nonlinear aspects of youthfulness and skeletal remodeling, and why, perhaps, infants have jowls. Plast Reconslr Surg. 1999;103:635-644.
7. Bosset S, Barre P, Chalon A, et al. Skin ageing: Clinical and histopathologic study of permanent and reducible wrinkles. Eur J Dermatol. 2002;23:247-252.
8. Fenske NA, Lober CW. Structural and functional changes of normal aging skin. J Am Acad Dermatol. 1986;15:571-585.
9. El-Domyati M, Attia S, Saleh F, et al. Inuinsic aging vs. photoaging: A comparative histopathological, immunohistochemical, and ul- uusunctural study of skin. Exj> Dermalol. 2002;11:398-405.
11. Little JW. Applications of the classic dermal fat graft in primary and secondary facial rejuvenation. Plast Reconstr Surg. 2002;109:788-804. ‘
12. Coleman SR. Structural fat grafts: The ideal filler? Clin Plast Surg. 2001;28:11 l-l 19.
13. StuzinJM, BakerTJ, BakerTM. Refinements in lace lifting: Enhanced facial contour using Vicryl mesh incorporated into SMAS fixation. Plast Reconslr Surg. 2000;105:290-301.
14. Jones DH. Semipermanent and permanent injectable fillers. Dermatol Clin. 2009;27:433-444.
15. Bucky LP, Kanchwala SK. The role of autologous fat and alternative fillers in the aging face. Plast Reconstr Surg. 2007;
120(6 Suppl):89S-97S.
16. Matros E, Momoh A, Yaremchuck MJ. The aging midfacial skeleton: Implications for rejuvenation and reconstruction using implants. Facial Plast Surg. 2009;25:252-259.
17. Flowers RS. Augmentation maxilloplasty. In: Terino EO. Flowers RS, eds. The Art of AUoplastic Facial Con touting. St. Louis: Mosby; 2000:129-150.
18. Warren SM. Spector JA, Zide BM. Chin surgery: The textured secured implant. A recipe for success. Plast Reconstr Surg 2007;120:1378-1385.
19. Yaremchuk MJ. Facial skeletal reconstruction using porous polyethylene implants. Plast Reconstr Surg. 2003;] 11:1818— 1827.
20. Stuzin JM. Restoring facial shape in face lifting: The role of skeletal support in facial analysis and midface soft-tissue repositioning. Plast Reconslr Surg. 2006;119:362-376.
21. Fattahi T. The prejowl sulcus: An important consideration in lower face rejuvenation. J Oral Maxillofac Surg. 2008;66: 355-358.