170 Commonwealth Avenue, Suite 101 Boston, MA 02116
Phone: (617) 726-5280
Changes in Eyebrow Position and Shape with Aging
Purpose
Lack of an objective goal for brow lift surgery may explain why several articles in the plastic surgery literature concluded that brow lifts produce eyebrows with shape and position![]() which are not aesthetically pleasing. By comparing eyebrow shape and position in both young and mature women this study provides objective data to plan forehead rejuvenating procedures.
which are not aesthetically pleasing. By comparing eyebrow shape and position in both young and mature women this study provides objective data to plan forehead rejuvenating procedures.
Methods
Two cohorts of women ages 20-30 and 50-60 were digitally photographed![]() to determine eyebrow position. Measurements were made from a horizontal plane between the medial canthi to three points at the upper eyebrow margin. Exclusion criteria included prior surgery, plucked eyebrows, or Botox.
to determine eyebrow position. Measurements were made from a horizontal plane between the medial canthi to three points at the upper eyebrow margin. Exclusion criteria included prior surgery, plucked eyebrows, or Botox.
Results
The eyebrow in the 20-30 year old group (n=36) measured 15.7, 19.8 and 21.3 mm above the medial canthus, pupil, and lateral canthus respectively. Lateral brow position was significantly higher than the mid-brow (p<.05). In the 50-60 year old group (n=34) the brow measured 19.1, 22.4 and 22.4 mm above the medial canthus, pupil, and lateral canthus respectively . At all three points, the brow was higher in older compared to younger subjects. This difference was significant at the medial and mid-brow (p<.05).
Conclusion
Unlike other areas of the body where there is descent of soft tissues, there is paradoxical elevation of eyebrows with aging. These findings explain why brow lifts may create an unnatural appearance and frequently fail to achieve the aesthetic ideal. Techniques that selectively elevate the lateral brow while repositioning the medial brow are preferred.
Introduction
In order to achieve consistent surgical outcomes with eyebrow rejuvenating procedures, aesthetic objectives for youthful brow shape and position need to be defined. In 1974 Westmore described characteristics of the ideal eyebrow as an arch where the brow apex terminates above the lateral limbus of the iris with the medial and lateral ends of the brow at the same horizontal level![]() 1. Freud and Nolan surveyed
1. Freud and Nolan surveyed![]() plastic surgeons and cosmetologists about their preferences for both eyebrow height and shape. Both groups preferred a medial eyebrow below or at the supraorbital rim with a shape that has an apex lateral slant2. Definitions of eyebrow aesthetics have been refined further by others, but taken together they provide a framework of aesthetic goals for surgeons to plan forehead rejuvenating procedures3.
plastic surgeons and cosmetologists about their preferences for both eyebrow height and shape. Both groups preferred a medial eyebrow below or at the supraorbital rim with a shape that has an apex lateral slant2. Definitions of eyebrow aesthetics have been refined further by others, but taken together they provide a framework of aesthetic goals for surgeons to plan forehead rejuvenating procedures3.
Despite studies which provide criteria for ideal brow aesthetics, reports in the literature suggest that brow lift procedures create brows with unnatural shape and position![]() . The disparity between practice and the ideal was documented in the second part of Freud and Nolan’s study2. The authors showed that brow lifts pictured in the medical literature frequently elevated medial eyebrows too high to a level
. The disparity between practice and the ideal was documented in the second part of Freud and Nolan’s study2. The authors showed that brow lifts pictured in the medical literature frequently elevated medial eyebrows too high to a level![]() above the supraorbital rim. In regards to brow shape, brow lift surgery was significantly more likely to create an apex medial or flat appearance than the desired apex lateral eyebrow contour. Gunter and Antrobus were concerned that the postoperative brow was over elevated creating a surprised and unintelligent look4. Through computer
above the supraorbital rim. In regards to brow shape, brow lift surgery was significantly more likely to create an apex medial or flat appearance than the desired apex lateral eyebrow contour. Gunter and Antrobus were concerned that the postoperative brow was over elevated creating a surprised and unintelligent look4. Through computer![]() image manipulation, the authors demonstrated that the preferred brow was one in which the original position was not elevated, but rather reshaped to a more gentle arch. They concluded that surgical brow lifts fail to provide the desired result because they tend to elevate the entire brow without lowering the medial segment. Trolius documented that brow lifts procedures were creating unnaturally high brows by examining postoperative measurements of patients who underwent sub-periosteal brow lifts with fixation56. He measured that brows continued to elevate an additional 2.5 mm between 1 and 5 years postoperatively. To achieve more natural results, the author revised his technique to eliminate fixation except in the most severe cases of brow ptosis. At the time these studies advanced understanding of brow aesthetics by demonstrating pitfalls of current surgical techniques, yet reports thereafter continued to define technical success of forehead rejuvenating procedures by the ability to the elevate brows with durable results7, 8.
image manipulation, the authors demonstrated that the preferred brow was one in which the original position was not elevated, but rather reshaped to a more gentle arch. They concluded that surgical brow lifts fail to provide the desired result because they tend to elevate the entire brow without lowering the medial segment. Trolius documented that brow lifts procedures were creating unnaturally high brows by examining postoperative measurements of patients who underwent sub-periosteal brow lifts with fixation56. He measured that brows continued to elevate an additional 2.5 mm between 1 and 5 years postoperatively. To achieve more natural results, the author revised his technique to eliminate fixation except in the most severe cases of brow ptosis. At the time these studies advanced understanding of brow aesthetics by demonstrating pitfalls of current surgical techniques, yet reports thereafter continued to define technical success of forehead rejuvenating procedures by the ability to the elevate brows with durable results7, 8.
Further support that forehead surgery creates brows with unnatural shape and height is substantiated by the fact that patients undergo brow lift reversal. Yaremchuk described a technique to restore brow appearance in 22 patients who underwent prior open or endoscopic brow lift procedures9. Patient complaints included high brows with unnatural shape and an increased spread between the medial brows. Through galea scoring, posterior scalp flap advancement and anchor suture fixation, brows were lowered on average 5 mm relative to an intercanthal line. With this technique the brow could be repositioned according![]() to patient preference, usually to an apex lateral configuration.
to patient preference, usually to an apex lateral configuration.
There is no clear explanation for the discrepancy between surgical results and a youthful brow appearance; however, one possibility is that little is understood about the aging process![]() that occurs at the eyebrow. Although anthropometric values in Caucasian women ages 19-25 were recorded by Farkas, objective documentation of changes in eyebrow height and shape with age are lacking10. Surgical studies document postoperative changes. Only a single report in the ophthalmology literature by van den Bosch demonstrates changes in female
that occurs at the eyebrow. Although anthropometric values in Caucasian women ages 19-25 were recorded by Farkas, objective documentation of changes in eyebrow height and shape with age are lacking10. Surgical studies document postoperative changes. Only a single report in the ophthalmology literature by van den Bosch demonstrates changes in female![]() brow height over time11. Measured at a single point above the pupil, the authors found that the mid-brow elevates with advancing age in both men and women. Improved understanding of the temporal changes that occur in brow position and shape may lead to better technique and outcomes.
brow height over time11. Measured at a single point above the pupil, the authors found that the mid-brow elevates with advancing age in both men and women. Improved understanding of the temporal changes that occur in brow position and shape may lead to better technique and outcomes.
Herein we describe changes in eyebrow position![]() and shape that occur over time by comparing cohorts of women ages 20-30 and 50-60. The intent is to better understand the aging process of the brow with a re-evaluation of current surgical techniques in light of these findings.
and shape that occur over time by comparing cohorts of women ages 20-30 and 50-60. The intent is to better understand the aging process of the brow with a re-evaluation of current surgical techniques in light of these findings.
Methods
Two random cohorts of Caucasian women ages 20-30 and 50-60 were prospectively photographed for the purpose of this study with the head in the upright and neck in neutral position. Digital photographs were captured with the forehead and eyebrows in a maximally relaxed position with the eyes open. All images included a metric ruler taped to the mid-forehead, just above the brows. Each eyebrow position was determined by measuring from a reference horizontal plane drawn between the medial canthi to vertical points on the upper brow margin at the medial canthus, pupil and lateral canthus. Using Adobe![]() imaging software (San Jose, CA) the photographed metric ruler was manipulated on screen to exactly measure these distances. Women were excluded if they had previous periorbital/forehead surgery, plucked the upper eyebrow margin, had significant ophthalmologic or neurologic disease or used botulinum toxin. All measurements were performed twice, once by each author (E.M. and J.A.G.), to ensure inter-rater reliability. Statistical analysis was performed by comparing group means with a t-test using standard statistical software, Intercooled Stata 6.0 (Stata Corp, College Station, TX). Values of p≤0.05 were considered significant.
imaging software (San Jose, CA) the photographed metric ruler was manipulated on screen to exactly measure these distances. Women were excluded if they had previous periorbital/forehead surgery, plucked the upper eyebrow margin, had significant ophthalmologic or neurologic disease or used botulinum toxin. All measurements were performed twice, once by each author (E.M. and J.A.G.), to ensure inter-rater reliability. Statistical analysis was performed by comparing group means with a t-test using standard statistical software, Intercooled Stata 6.0 (Stata Corp, College Station, TX). Values of p≤0.05 were considered significant.
Results
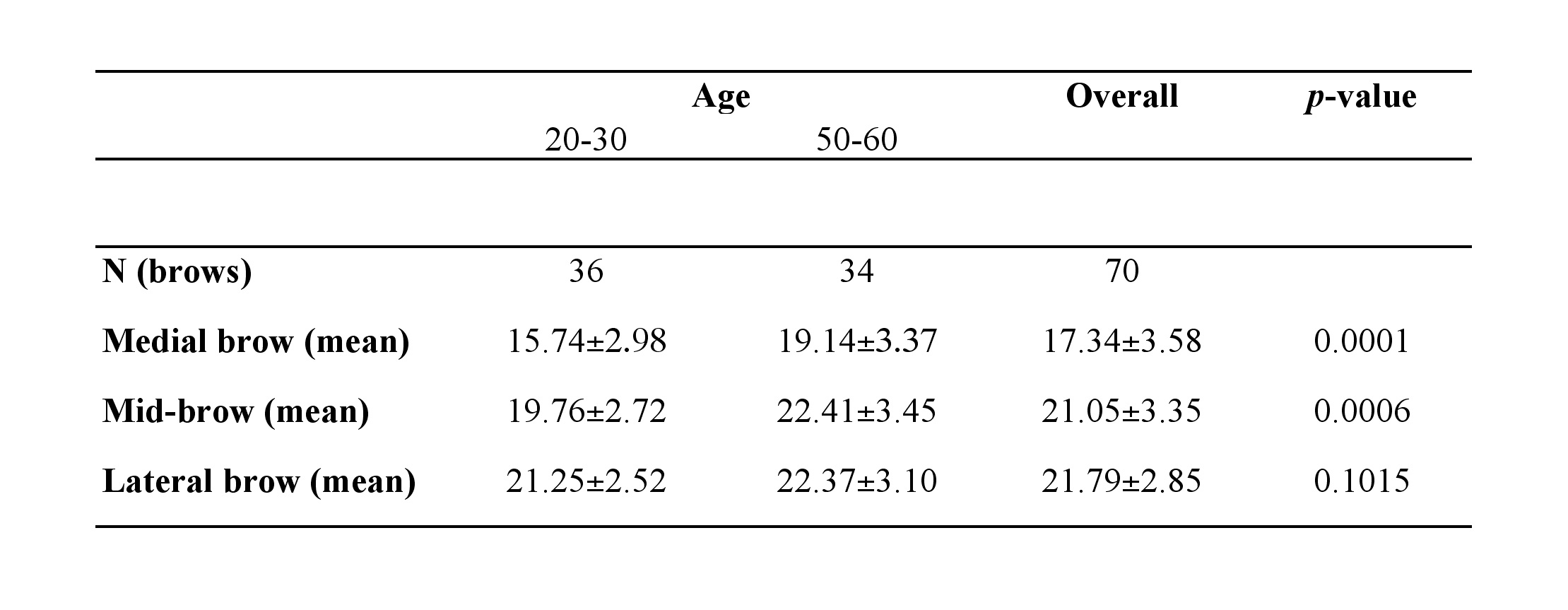
As shown in Table 1, position of the upper eyebrow margin in the 20-30 year old group (n=36), measured 15.7 mm, 19.8 mm and 21.3 mm above the medial canthus, pupil, and lateral canthus respectively. The lateral brow position measured significantly higher than the mid-brow (p<.05). In the 50-60 year old group (n=34) the upper brow measured 19.1 mm, 22.4 mm and 22.4 mm above the medial canthus, pupil, and lateral canthus respectively (Table 1). For each of the three points measured, the brow was at a higher in position in the older than the younger subjects (Figure 1). This difference was statistically significant at the medial and mid-brow positions (p<.05). Typical results for patients from each cohort are shown in Figure 2.
 Discussion
Based on what is known about the aging process![]() in other soft tissue structures of the body, it is logical to believe that eyebrows descend over time. On the contrary, there is evidence in the literature supporting current findings that brows elevate with age. van den Bosch in an effort to better understand age related eyelid pathology such as ectropion and dermatochalasis, studied the affects of aging on the eyelid, eyeball, and eyebrow11. In a cohort study of 320 subjects, which included men and women ages 10 to 89, the authors measured that eyebrow height over the pupil increased significantly with advanced age in both genders. Eyebrow position was higher overall in women than in men. In contrast, a study by Goldstein and Katowitz of 222 males demonstrated that eyebrow position above the pupil and lateral canthus did not increase, but remained the same over time12. Design of these studies differs from the current, yet they objectively document that brows ascend, or at the very least, remain level
in other soft tissue structures of the body, it is logical to believe that eyebrows descend over time. On the contrary, there is evidence in the literature supporting current findings that brows elevate with age. van den Bosch in an effort to better understand age related eyelid pathology such as ectropion and dermatochalasis, studied the affects of aging on the eyelid, eyeball, and eyebrow11. In a cohort study of 320 subjects, which included men and women ages 10 to 89, the authors measured that eyebrow height over the pupil increased significantly with advanced age in both genders. Eyebrow position was higher overall in women than in men. In contrast, a study by Goldstein and Katowitz of 222 males demonstrated that eyebrow position above the pupil and lateral canthus did not increase, but remained the same over time12. Design of these studies differs from the current, yet they objectively document that brows ascend, or at the very least, remain level![]() with advancing age.
with advancing age.
The current findings also provide objective measurements about changes in eyebrow shape that occur with aging. In the 20-30 year old cohort, the lateral brow was positioned![]() significantly higher than the mid-brow (Table 1). The medial eyebrow measured at the lowest height of any brow segment in either age group. These measurements describe the youthful eyebrow reported as the aesthetic ideal and serve as the goal for forehead rejuvenating procedures2, 13. In contrast, the 50-60 patients have lateral and mid-brow segments at similar heights, creating a flat appearance or in some cases an apex medial configuration
significantly higher than the mid-brow (Table 1). The medial eyebrow measured at the lowest height of any brow segment in either age group. These measurements describe the youthful eyebrow reported as the aesthetic ideal and serve as the goal for forehead rejuvenating procedures2, 13. In contrast, the 50-60 patients have lateral and mid-brow segments at similar heights, creating a flat appearance or in some cases an apex medial configuration![]() (Figure 2). Although aging of the lateral brow is often referred to as ptosis, a more accurate term to describe the process is pseudoptosis, since the medial and middle brows ascend more than the lateral brow.
(Figure 2). Although aging of the lateral brow is often referred to as ptosis, a more accurate term to describe the process is pseudoptosis, since the medial and middle brows ascend more than the lateral brow.
Multiple mechanisms may explain why brows paradoxically elevate with advancing age. “Spastic frontalis syndromeâ€, described Ramirez, refers to chronic activation of the frontalis muscle![]() with associated elevation of the brow/eyelid complex to overcome clinical or sub-clinical levator system weakness14. Reportedly this compensatory mechanism leads to a higher and more arched brow shape in people as they age. Further support for levator aponeurosis dis-insertion was supplied by van den Bosch who objectively documented that aging is associated with an elevated upper eyelid skin crease11. An alternative explanation for brow elevation comes from the fact that patients chronically elevate their brows to reduce visual field obstruction from excess upper eyelid skin. Trolius noted that after blepharoplasty, the stimulus for frontalis contraction is alleviated which in turn leads to eyebrow descent5. In 10 patients who underwent upper blepharoplasty alone he measured that brow height decreased postoperatively on average 3.3, 3.6 and 3.3 mm at the medial canthus, pupil and lateral canthus respectively. The author recommends
with associated elevation of the brow/eyelid complex to overcome clinical or sub-clinical levator system weakness14. Reportedly this compensatory mechanism leads to a higher and more arched brow shape in people as they age. Further support for levator aponeurosis dis-insertion was supplied by van den Bosch who objectively documented that aging is associated with an elevated upper eyelid skin crease11. An alternative explanation for brow elevation comes from the fact that patients chronically elevate their brows to reduce visual field obstruction from excess upper eyelid skin. Trolius noted that after blepharoplasty, the stimulus for frontalis contraction is alleviated which in turn leads to eyebrow descent5. In 10 patients who underwent upper blepharoplasty alone he measured that brow height decreased postoperatively on average 3.3, 3.6 and 3.3 mm at the medial canthus, pupil and lateral canthus respectively. The author recommends![]() careful analysis of brow position prior to blepharoplasty otherwise patients can look worse postoperatively. Taken together, there is plausible mechanistic data to support brow elevation with aging.
careful analysis of brow position prior to blepharoplasty otherwise patients can look worse postoperatively. Taken together, there is plausible mechanistic data to support brow elevation with aging.
Anatomical evidence for changes in brow position![]() and shape with age are provided in detailed cadaver dissections by Knize15. His study showed that beyond the temporal fusion line, where the frontalis muscle
and shape with age are provided in detailed cadaver dissections by Knize15. His study showed that beyond the temporal fusion line, where the frontalis muscle![]() insertion ends laterally, there is no upward vector to counteract the gravitational forces on the soft tissue temporal mass. The variable position of where the fusion plane terminates laterally provides explanation for heterogeneity of lateral brow positioning amongst females. Finally, the presence of a lateral orbital retaining ligament between the superficial temporal fascia and the zygomaticofrontal suture fixes the lateral eyebrow preventing movement to a degree equivalent to the medial brow. Tethering of the lateral brow with absence of frontalis in this area, may explain why the lateral brow did not measure at significantly different heights in young and mature women (Table 1).
insertion ends laterally, there is no upward vector to counteract the gravitational forces on the soft tissue temporal mass. The variable position of where the fusion plane terminates laterally provides explanation for heterogeneity of lateral brow positioning amongst females. Finally, the presence of a lateral orbital retaining ligament between the superficial temporal fascia and the zygomaticofrontal suture fixes the lateral eyebrow preventing movement to a degree equivalent to the medial brow. Tethering of the lateral brow with absence of frontalis in this area, may explain why the lateral brow did not measure at significantly different heights in young and mature women (Table 1).
Standard brow lift procedures are performed based on the premise that brows naturally descend with advanced age. Data from this study objectively demonstrate that brows, in particular the medial and mid-brow segments, elevate with age and explains why current brow lift procedures, which tend to preferentially elevate the medial brow, create an unnatural appearance5,8. Based on these findings a reappraisal of current brow-lift techniques is warranted. First, since there is heterogeneity in anatomy and how brows age, a cookie cutter approach to brow rejuvenation should be abandoned with operations tailored based on preoperative findings and patient preference. Most patients require brow reshaping by lowering of the medial brow segment and restoration of the brow apex to above the lateral limbus of the iris. In order to achieve differential positioning of the eyebrow segments, an open coronal approach is recommended as it allows more control than endoscopic techniques. To ensure placement of the medial brow in the desired position it can be fixed to the frontal bone by a Mitek anchor with the needle passed through the backside of the scalp flap9. With this method, the medial brow segment is lowered and shifted either medially or laterally depending upon preoperative anatomy. The apex lateral configuration can be restored by suturing the galea of the scalp flap, corresponding to the tail of the brow, to the deep temporal fascia. Preservation of the corrugator muscles![]() as a secondary maneuver prevents medial brow spread and maintains a downward vector at the medial brow to counterbalance upward motion by the frontalis. Persistent forehead and glabellar rhytids are subsequently treated with botulinum toxin as needed16,17. Finally, the effect of concomitant blepharoplasty, which tends to lower the brow by alleviating the need to elevate excess upper eyelid skin, needs to be considered.
as a secondary maneuver prevents medial brow spread and maintains a downward vector at the medial brow to counterbalance upward motion by the frontalis. Persistent forehead and glabellar rhytids are subsequently treated with botulinum toxin as needed16,17. Finally, the effect of concomitant blepharoplasty, which tends to lower the brow by alleviating the need to elevate excess upper eyelid skin, needs to be considered.
Unlike other areas of the body where there is relative descent of soft tissues, there is, on average, a paradoxical elevation of the eyebrow with aging in women. The apex lateral contour of the youthful brow is transformed into a flattened brow (apex neutral) over time. These findings explain why current brow lift procedures fail to achieve the aesthetic ideal and provide a rationale for lowering previously surgically elevated brows. When aiming to rejuvenate the forehead region![]() , a youthful brow contour is more likely to be achieved if it repositioned strategically along its course rather than simply “elevatedâ€. Moving forward, the term brow lift should be substituted for descriptive terms such as foreheadplasty or browpexy which more accurately describe the necessary operation.
, a youthful brow contour is more likely to be achieved if it repositioned strategically along its course rather than simply “elevatedâ€. Moving forward, the term brow lift should be substituted for descriptive terms such as foreheadplasty or browpexy which more accurately describe the necessary operation.
Table 1
Â
Figure 1
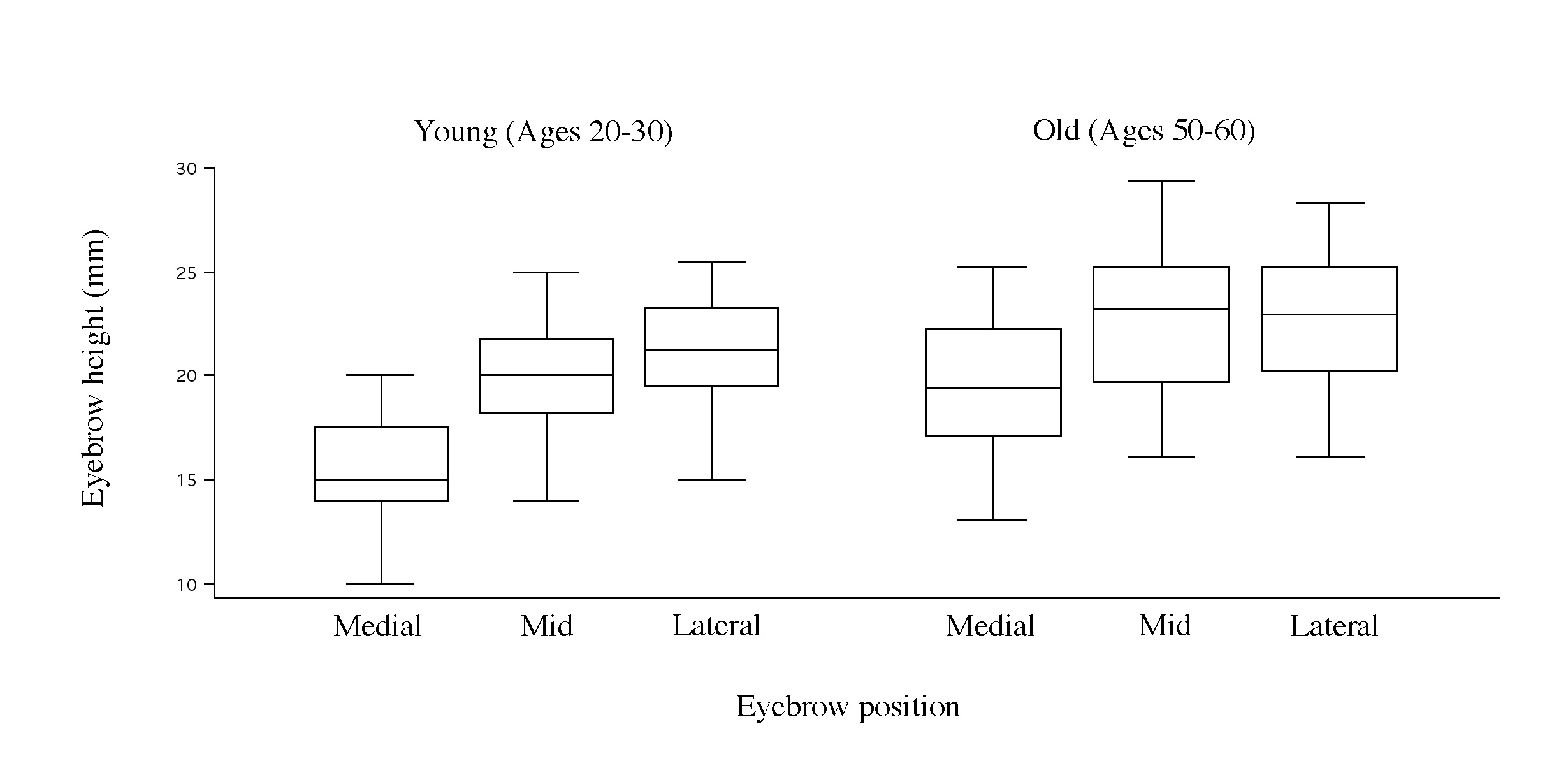
Legend: Box-plot representation of eyebrow height in young and older women. At each of the three positions![]() , the brow is higher in older than younger women. Relative position of the box plots in younger women shows an apex lateral shape to the brow, whereas in older women the lateral brow appears flattened.
, the brow is higher in older than younger women. Relative position of the box plots in younger women shows an apex lateral shape to the brow, whereas in older women the lateral brow appears flattened.
Figure 2
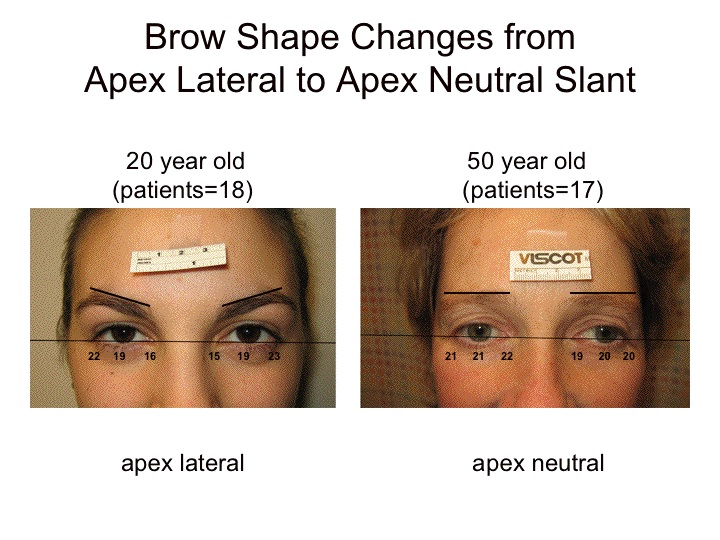
Legend: Typical results for patients from each cohort are shown. Younger patients have a medial brow which is low, with an apex lateral configuration![]() . Older patients have an elevated medial and middle brow which contributes to a flattened appearance. Measurements to the top of the brow margin are shown for each point measured.
. Older patients have an elevated medial and middle brow which contributes to a flattened appearance. Measurements to the top of the brow margin are shown for each point measured.
References
- Westmore M. Facial cosmetics in conjunction with surgery. Paper presented at: Aesthetic Plastic Surgical Society Meeting. May 1974.
- Freund RM, Nolan WB, 3rd. Correlation between brow lift outcomes and aesthetic ideals for eyebrow height and shape in females
 . Plast Reconstr Surg. 97: 1343, 1996.
. Plast Reconstr Surg. 97: 1343, 1996. - Schreiber JE, Singh NK, Klatsky SA. Beauty Lies in the “Eyebrow” of the Beholder: A Public Survey of Eyebrow Aesthetics. Aesthetic Surgery Journal. 25: 348, 2005.
- Gunter JP, Antrobus SD. Aesthetic analysis of the eyebrows. Plast Reconstr Surg. 99: 1808, 1997.
- Troilius C. Subperiosteal brow lifts without fixation. Plast Reconstr Surg. 114: 1595, 2004.
- Troilius C. A comparison between subgaleal and subperiosteal brow lifts. Plast Reconstr Surg. 104: 1079, 1999.
- Behmand RA, Guyuron B. Endoscopic forehead rejuvenation: II. Long-term results. Plast Reconstr Surg. 117: 1137, 2006.
- Swift RW, Nolan WB, Aston SJ, Basner AL. Endoscopic Brow Lift: Objective Results After 1 Year. Aesthetic Surgery Journal. 19: 287, 1999.
- Yaremchuk MJ, O’Sullivan N, Benslimane F. Reversing Brow Lifts. Aesthetic Surgery Journal. 27: 367, 2007.
- Farkas LG, Hreczko TA, Katic MJ. Craniofacial Norms in North American Caucasians from Birth to Adulthood. Appendix A. Antrhopometry of the Head and Face. 2nd Ed. New York: Raven Press: 241, 1994.
- van den Bosch WA, Leenders I, Mulder P. Topographic anatomy of the eyelids, and the effects of sex and age. Br J Ophthalmol. 83: 347, 1999.
- Goldstein SM, Katowitz JA. The male eyebrow: a topographic anatomic analysis. Ophthal Plast Reconstr Surg. 21: 285, 2005.
- Ellenbogen R. Transcoronal eyebrow lift with concomitant upper blepharoplasty. Plast Reconstr Surg. 71: 490, 1983.
- Ramirez OM. Discussion of Trolius C. Subperiosteal browlifts without fixation. Plast Reconstr Surg. 114: 1604, 2004.
- Knize DM. An anatomically based study of the mechanism of eyebrow ptosis. Plast Reconstr Surg. 97: 1321, 1996.
- Guyuron B, Huddleston SW. Aesthetic indications for botulinum toxin injection. Plast Reconstr Surg. 93: 913, 1994.
- Fagien S. Botox for the treatment of dynamic and hyperkinetic facial lines and furrows: adjunctive use in facial aesthetic surgery. Plast Reconstr Surg. 103: 701, 1999.
Leave Comments
You must be logged in to post a comment.